There is much to be said for systems thinking or a systems-informed approach to key tasks such as evaluation. If the policy problem is complex, then we would not expect a single shot solution to work as intended in a linear or even straightforward way. If so, traditional ways to assess success or failure would be inappropriate. This broad argument has some traction, even in places associated with traditional evaluations in relation to policy cycles (such as the UK Treasury and its Magenta book supplement). However, just as systems thinking can mean 10 different things (and refer to two contradictory approaches), systems evaluation can involve very different tasks. Beware the possibility of contradictory ideas emerging from this process.
What exactly is a systems approach?
Systems thinking relates to the idea that key aspects of policy and policymaking resemble the complex systems that we find in nature, society, the brain, and information technology. Here, complex does not mean complicated. Rather, complex systems are greater than the sum of their parts, and exhibit non-linear dynamics, and prompt outcomes that emerge without central control.
Crucially, this argument can be related to many different types of policy relevant systems, including:
Complex policy problems. Policy problems are multi-faceted or inter-related, difficult to break down into specific parts, and not amenable to simple solutions.
Complex policy processes. Policymaking systems resemble complex systems
Complex policy mixes. ‘Policy’ is actually a policy mix, or large collection of policy instruments. The overall impact, of directing many policy instruments at one or more problems, is difficult to control or even predict. Overall policy incoherence may be a feature of such complexity.
In that context, I argue that people may be conflating three separate issues in the name of systems thinking evaluation, potentially with ironic unintended consequences. I make the distinction as follows:
Systems evaluations focusing on a complex policy problem, such as obesity. The aim is to identify the interconnectedness of the policy problem, such as to connect poverty, education, safe and healthy spaces, access to healthy food, commercial incentives, and so on. If so, we can adopt a ‘whole systems’ perspective to try to understand the problem, respond, and seek more meaningful ways to evaluate. This perspective may also be used to reject simplistic descriptions of problems (e.g. scroll down this page to see the ‘obesity system atlas’).
Systems evaluation focusing on a policymaking or governance problem, such as a lack of concerted attention or effective collaboration to solve a problem. The aim is to identify the interconnectedness of policy processes, such as: who is responsible for what, how does it all add up to systemic action, and what would a good policymaking system look like? Or, we may try to provide a map of policymaking responsibilities spread across levels of government (e.g. national/local) or sectors (e.g. health, education, transport, environment). If we intervene to change how we do things around here, we can assess the impact on things like levels of policy coherence or policymaking integration or cooperation. This perspective may also be used to counter the idea that one single centre of government can change things from the top-down.
Systems evaluation focusing on the overall impact of the policy mix. If many organisations use many instruments, is the policy mix coherent? Does each instrument reinforce or undermine the other? If we find limited success in relation to one instrument, is the problem really the other instruments? Or the delivery of the same instruments in different or unintended ways?
The potential irony arises if we recommend systems thinking in relation to one aspect but take a rather linear approach to others. Here, the classic mistake is to apply systems thinking to a problem but then act as if the solution can be produced by one central authority in a straightforward manner in a policymaking system. It is strange to see policy recommendations about problem complexity that do not recognise policymaking complexity. Why spend so much time identifying the interconnectedness of problems only to propose simple accounts of the responsibility for solutions?
One answer worth pursuing (because it represents a point of common ground) is that lots of people are inspired by Donella Meadows to find ‘leverage points’, ‘where a small shift in one thing can produce big changes in everything’. Yet, Meadows notes there are ‘no cheap tickets’ to a full understanding of systems. In our case, there is no easy way to find leverage points in complex policymaking systems, even if you have a good sense of a complex problem.
In this piece, Professor Catherine Durose, Professor Sarah Ayres FAcSS, Professor John Boswell FAcSS, Professor Paul Cairney FAcSS, Dr Ian C Elliott, Professor Matthew Flinders, Professor Steve Martin and Professor Liz Richardson discuss how Positive Public Policy (PoPP) can drive performance improvements, save money, foster early interventions, align networks, and build capacity and momentum for more effective government.
Policy takeaways:
1. A different approach to policy-making is urgently required to address the chronic problems, complex crises and emerging challenges facing the UK.
2. Positive Public Policy (PoPP) encourages learning from success and failure to inform strategic, systemic and participatory approaches to government.
3. PoPP can drive performance improvements, save money, foster early interventions, align networks, and build capacity and momentum for more effective government. But to achieve it we need to find new ways to connect researchers with policymakers and practitioners across the UK.
Traditional approaches to policymaking struggle to deal with chronic problems such as health inequalities, growing crises such as the climate emergency, and emerging issues such as advances in artificial intelligence (AI). There is widespread acknowledgement of the need to transform the inner workings of government in order to rise to these challenges. The incoming UK government will be faced with an intimidating to-do list twinned with severe pressure on public spending. However, this presents an opportunity to create a more agile, coherent, responsive and effective approach to public policy. To assist in meeting this challenge, Positive Public Policy offers a coherent vision of how to achieve this and improve real-world outcomes.
The last two decades have witnessed a prolonged permacrisis during which the UK government has bounced reactively from financial crisis and austerity, through to Brexit, COVID-19, a cost-of-living crisis and increasing evidence of falling levels of public trust in politicians and in politics, matched by rising and increasingly concerning levels of anti-political sentiment. Our policymaking has been characterised by the dominance of a narrow range of perspectives, an emphasis on short-term outcomes and the backstory of the depletion of good governance. A limited form of Westminster-style democratic accountability continues to skew policy attention and resources to short-term and centralised approaches which have starkly revealed that what makes for ‘good’ politics, often fails to produce good policymaking.
Yet, there is shared recognition that business-as-usual in policy and policymaking is insufficient in a context of intense inequality, radical uncertainty, complexity and heightened polarisation. Further, there is a need to boost strategic policymaking capacity in order to live up to = the principles of effective government including the importance of being responsible and accountable, future-oriented, preventative, decentralised, co-productive, integrated, evidence-informed and equitable. The UK government recognised this in the Declaration on Government Reform published in July 2021. The General Election potentially offers a window of opportunity for meaningful change, but also a context of real challenge. So how can positive change be facilitated?
Effective government may be understood as a ‘magical’ concept: common sense enough to achieve political support, but evading a clear sense of how it can be achieved. It is rare to find a coherent account of how government can manage competing drivers. For example, governments centralise to avoid postcode lotteries, but decentralise to reflect local circumstances; they seek integration and coherence but create policy from within departmental ‘silos’. Reformers face significant obstacles. Policymakers frequently operate in complex systems, are constrained by a lack of resources and, are regularly blindsided by events, the electoral cycle, media stance or party politics. It is not possible to simply pull levers to make reforms happen. Add this to a sense that political capital is required across a range of priorities, and it is clear why simply muddling through becomes the default.
However, a different way of thinking about a ‘magical’ concept is that it provides an important port in a storm, an ideal to aspire to, and is useful in navigating challenging environments. In this sense, ‘effective government’ becomes a useful aspiration. But how can we achieve it? Aligning with the growing ‘Positive Public Policy’ (PoPP) movement, we challenge the assumption that public policy is doomed to fail and instead focus attention on learning from both failed and successful public policy. In doing so, we want to point to change and offer ways to learn from and share lessons of experiences from the past and other contexts.
PoPP embraces a range of approaches aiming to facilitate effective government and policymaking. Some are relatively new while others have been discussed and studied for decades without realising their full potential. These include the concept of the strategic state, systems-thinking, place-based approaches, evidence-informed government, public participation, and behavioural public policy. What connects these approaches is (i) an appreciation of the complexity and inter-connected nature of policy contexts, (ii) a belief in the capacity of collective action to address shared challenges, and (iii) a commitment to the collection, synthesis and application of different forms of knowledge. Each has been tested and is underpinned by an accumulation of evidence – including, good practice, frameworks, case studies, and policy learning – and together they provide a coherent reform agenda and a fresh portfolio of ways of designing and delivering high-performing public policy.
Years of instability in UK government have eroded underlying capacity for reform. The General Election will be conducted against the backdrop of financial stress across government, and no reform is cost-free. Will an incoming government give priority to getting its own house in order? And taking the leap of faith reform requires? Positive Public Policy embodies the vision of real change to drive change to address the significant social, economic and environmental challenges we face. It provides a range of approaches, tools and methods for designing and delivering effective public policy, and the clear, coherent and sustainable story of reform required to lower barriers to change and to leveraging resources.
What we need is the political will and sustained capacity to trial and test the insights of Positive Public Policy in a UK context, and this in turn calls for investment in connective and catalysing engagement opportunities between researchers and policymakers. There’s an urgent need to connect the positive public policy academic community with practitioners at scale in order to help constitute the policymaking tools that governments can use as they grapple with the ‘art of the possible’ to translate lofty ideals into practices that might work in their own context. Now is the time to attract and devote resources towards trialling, tracking and evaluating experimentation in more future-oriented, holistic, and more participatory approaches to government.
About the authors
Catherine Durose is Professor of Public Policy, and Co-Director of the Heseltine Institute for Public Policy, Practice and Place at the University of Liverpool. She is recognised as a leading expert on urban governance and public policy, with a particular focus on how citizens and communities can engage in the policy and decision-making that affects their everyday lives.
Sarah Ayres is Professor of Public Policy and Governance at the University of Bristol. Sarah’s work has explored the complexities of devolution and city governance by exploring the inter-play between formal and informal structures, processes and outcomes. Her research has provided critical insights into how ‘informal’ decision making, i.e. what happens behind closed doors between political elites, has shaped devolution in the UK. This research has made a distinctive contribution by examining the impact of so-called ‘informal governance’ on different aspects of mainstream governance theory, including political innovation, democracy, policy effectiveness and the creation of public value.
John Boswell is Professor of Politics at the University of Southampton. His research and teaching are in democratic governance, public policy and public administration, and he is one of the co-directors of the Centre for the South, a regional policy think tank. His interests centre around contemporary issues and themes in democratic governance and public policy, with his research being generally qualitative and interpretive in nature.
Paul Cairney is Professor of Politics and Public Policy at the University of Stirling. He is a specialist in British politics and public policy, often focusing on the ways in which policy studies can explain the use of evidence in politics and policy, and how policymakers translate broad long term aims into evidence-informed objectives (for example, The Politics of Evidence-Based Policymaking, 2016).
Ian C Elliott is Senior Lecturer in Public Policy and Administration at the Centre for Public Policy at the University of Glasgow and the Co-Editor-in-Chief of Public Administration and Development. His research includes work on strategy in government, public leadership and organisational change.
Matthew Flinders is Professor of Politics and the Founding Director of the Sir Bernard Crick Centre at the University of Sheffield. He is also Vice-President of the Political Studies Association and Chair of the Universities Policy Engagement Network. A former ESRC board member, he led the 2020 national review of research leadership – Fit for the Future – and is currently working with UKRI in relation to talent management and research culture investments. A former special advisor in both the House of Lords and House of Commons, he specialises in theoretically informed policy-relevant research and is a former ESRC National Impact Champion.
Steve Martin is Professor of Public Policy and Management at Cardiff University and Director of the Wales Centre for Public Policy. Prior to his current role he founded and directed the Centre for Local & Regional Government Research at Cardiff. Steve’s research focuses on evidence-informed policy, local government policy and public service improvement. He chaired the UK Government’s Expert Panel on Local Government and has acted as an adviser to the European Commission, UK, Scottish and Welsh Governments.
Liz Richardson is Professor of Public Administration at the University of Manchester. Her research interests include participatory urban governance; local politics and local government; public services; and public policy. She has an interest in methodological innovation including participatory research approaches, and experimental methods.
Douglas, S., Schillemans, T., ‘t Hart, P., Ansell, C., Bøgh Andersen, L., Flinders, M., Head, B., Moynihan, D., Nabatchi, T., O’Flynn, J. and Peters, B.G. (2021) ‘Rising to Ostrom’s challenge: an invitation to walk on the bright side of public governance and public service’, Policy Design and Practice, 4:4, 441-451 https://doi.org/10.1080/25741292.2021.1972517
The term ‘social policy’ describes a wide range of concerns, including policy and processes regarding ageing, children, families, education, crime, health, housing, social security and welfare, and social care. A key theme is the study of inequalityand inequalities, which is pertinent in the UK owing to the country’s highly unequal social and political system. Policy action could help to address inequalities, such as over class, sex and gender, race and ethnicity, religious, sexuality, disability, and age. Political protest may help to challenge or draw attention to inequalities and demand action to address them. We use our three lenses to these and related issues:
Policy analysis: How should we analyse inequalities as interconnected policy problems?
Critical policy analysis: Who wins and loses from these developments, and how should we (and policymakers) respond?
The UK has a long history of protest, including against the Poll Tax; Section 28, University tuition fees in England; and government inaction following the Grenfell Fire in 2017. There have also been protests against international phenomena, including led by women over Donald Trump’s election as US President; and a UK variant of the US-formed ‘Black Lives Matter’. These protests emphasise the importance of political activity outside of the UK’s ‘Westminster’ model. Their proponents describe them as essential, while their opponents often characterise them with reference to ‘riots’ or disruption to a ‘law abiding’ public.
Policy analysis: Defining, addressing, and solving inequalities
We explore how policymakers define, identify solutions to, and attempt to solve inequalities:
Inequality may be identified as a ‘wicked’ problem, with intense contestation over issues such as the severity and urgency of inequalities; their cause, and; which inequalities can be tolerated, or might even be considered just.
Some solutions identify structural causes or ‘social determinants’, and propose redistribution, regulation, or a challenge to austerity. Some propose ‘joining up’ government or ‘mainstreaming’ policies to reflect the cross-cutting nature of problems and mitigate against incoherent responses.
Inequalities are plagued by contestation and ambiguity, with anti-inequality strategies highlighting the potential for high state intervention but a tendency to favour modest intervention, or policies which create more inequalities in practice.
Overall, equity policies are difficult to sustain because
policymakers make broad claims for policy changes in the name of equity, but in practice undermine them (see the Conservative government’s “Levelling Up” agenda),
they quickly find out that these objectives clash with other, more established and higher priority policies (such as the need to maintain economic growth or maintain electoral support from key voter groups) and
most policymakers are unwilling or unable to engage in a direction or step-change in established patterns of policymaking.
The result is too often one of eye-catching promises, followed by modest or no policy change.
Policy studies: the London ‘riots’ in 2011
The events of August 2011 in London help to explore how each aspect of inequalities policy analysis are contested. All can agree that Mark Duggan, a 29 year old British man of mixed race, was killed in Tottenham North London by an on-duty Metropolitan Police officer. Beyond this, every other aspect of what occurred is contested, including:
The cause of the killing. The Metropolitan Police claimed Duggan was shot because he was armed and dangerous. Their critics note that this fits a pattern of racist and discriminatory behaviour.
What happened next. Some described a heavy-handed response to protests against police violence, others described ‘rebellions’ or ‘counter conduct’. Other voices, which predominated, characterised it as ‘rioting’, marked by ‘looting’, ‘violence’, and ‘disorder’, summed up by Prime Minister David Cameron’s comment that these were “riots, pure and simple”.
Whether the riots resulted from structural causes such as inequality, police racism, and austerity on the one hand, or criminality, family breakdown, and moral shortcomings on the part of the rioters on the other.
Policymakers used the criminality narrative to pursue not only a punitive policing and legal response, but also to scale up the ‘Troubled Families’ programme. The latter sought to ‘turn around’ families with ‘entrenched issues’ (such as ‘worklessness’, ‘anti-social behaviour’, and ‘truancy’), in line with David Cameron’s diagnosis of a ‘Broken Society’ and his prescription of a ‘Big Society’.
Critical Policy Analysis
Critical policy analysis combines research to highlight inequalities with advocacy to defend or support marginalised groups. Critical race theory (CRT) emerged to challenge entrenched white supremacy in political, scholarly, academic, and other public institutions, and support intersectional approaches.
To its critics in the US and UK (including in government), CRT represents a threat to politics and society. The UK Government’s alternative focus on ‘race and ethnic disparities’ asked how to advance the ‘progress’ won by the struggles of the past 50 years. This approach sought to dismiss concerns about institutional and systemic racism in favour of a more benign framing, and seemed to justify existing approaches rather than to prefigure substantial policy change.
Inequalities and the Westminster and Complex Government stories
Critics of limited policy progress to reduce inequalities use the Westminster story to hold senior policymakers responsible for failing to act: if they could be bothered to learn about the social determinants of policy problems, and exhibited some political will, they could reduce inequalities in the UK. Instead, they favour platitudes and make problems worse by individualising complex social issues. The complex government story helps to explain the inevitable lack of progress to ‘join up’ policy and policymaking to reduce inequalities. Modern governments may put their faith in ‘holistic’ policymaking to take forward cross-cutting policy agendas to tackle spatial, educational, health or other forms of inequalities, but generally find that their reforms don’t live up to expectations.
That question was the title of an op-ed that I wrote for the Scotsman on 11 July 2000 about compensation for people with haemophilia infected by hepatitis-C through blood products in the NHS. The answer turned out to be decades, largely because the UK government has always resisted the idea of compensation for treatment by the NHS, but with exceptions in relation to HIV or with reference to wider financial support by the state.
Below, I reproduce that Scotsman op-ed to provide background on UK government resistance to compensation, then link to some resources on how the issue played out in Scotland in the early years of devolution. In short, it became an intergovernmental relations issue when (1) there was pressure on the Scottish Government (then ‘Executive’) to respond, but (2) the UK government resisted successfully the idea that the Scottish Government could go its own way.
‘How long must these sufferers wait for the compensation they deserve?’
“SCOTTISH haemophiliacs are eagerly awaiting the results of a government investigation into the issue of hepatitis-C infection through blood products. However, this is an issue which should concern us all, not only because of the extent of suffering this type of infection causes, but also because it strikes at the heart of the whole question of compensation within the NHS.
It is also fitting that this issue should raise its head during the annual international AIDS conference, since – at least politically – the similarities between hep-C and HIV infection are uncanny. So how do we explain why HIV -infected haemophiliacs were compensated over ten years ago and yet haemophiliacs infected by hepatitis-C have had to wait until now even to hear if they have a case?
HIV and hepatitis-C are both particularly serious infections. The former – unless we believe Professor Duesberg – causes AIDS and diminishes the body’s ability to overcome subsequent infections, however slight. The latter, in the long term, causes chronic liver disease and cirrhosis. Either infection combined with haemophilia causes devastation among sufferers, their families and their friends. So why does one particular sufferer receive compensation and another doesn’t?
To put it bluntly, the main reason may well be that hepatitis-C is far less likely to capture the imagination of the public, Parliament or the government of the day. Hepatitis-C, unlike HIV, is only transmitted through blood and so its incidence within the general public is much less likely. Rather, on the whole it will only affect haemophiliacs and intravenous drug users. It is associated with minorities and/or deviance. It is unlikely to be able to maintain attention for any particular length of time. This is the key to the difference – HIV caught the public’s imagination because it was, and still is, presented as an infection which did or does not discriminate. It is transmitted sexually; it is transmitted through blood; it is transmitted from mother to baby; for a while it was thought that it might even be transmitted through saliva. It therefore affects us all and, albeit to a lesser and lesser extent, HIV continues to grab the headlines.
It is this crucial difference which informs much of the process of compensation. In both cases successive British (and now Scottish) governments attempted to deny responsibility for the compensation of those infected through blood products. However, this was largely unsuccessful with HIV because the issue just did not go away.
When, in the early Eighties, ministers denied the links between blood products and HIV, newspapers were filled with scientific reports which suggested otherwise. When ministers tried to delegate responsibility for HIV infections to haemophiliac specialists or health authorities, Parliament asserted its right to hold them to account. When the government accepted both the links and the responsibility, but not the need for compensation, the continuous public reaction forced a U-turn in government policy. And finally when the government accepted the need to compensate, but only those haemophiliacs who constituted a “special case”, it was again defeated by the threat of legal action supported by media, British Medical Association and MPs.
But is this likely to happen in the case of hepatitis-C? While those affected may take hope from the fact that the Scottish executive is finally taking their plight seriously, there is still one major obstacle to the granting of compensation – precedent. The most striking aspect of HIV in this regard was that the government could not afford to grant “no-fault” compensation to anyone suffering at the hands of the NHS for fear of opening the floodgates for a succession of similar claims. So, when granting a “trust fund” to HIV -infected haemophiliacs, it argued that these were “wholly exceptional circumstances”, with the implication that such compensation (although it was never termed as such) would never be repeated.
On the other hand, there is hope to be taken from this process, not least because since then the government has argued that those non-haemophiliacs infected with HIV through blood products were “also a very special case.” It seems, then, that to be successful a group just has to agree that what it is receiving is an exceptional compassionate payment rather than “compensation”.
More seriously, whether the government likes it or not, it has already set the precedent for haemophiliacs, when it recognised in 1990 that theirs were “wholly exceptional circumstances” and that haemophilia combined with another serious condition merited compensation, however this is phrased.
The government therefore has a responsibility to treat hepatitis-C sufferers in the same way as it treated those infected with HIV, irrespective of the findings of its investigation”
Attention in the Scottish Parliament (2001)
For example, the Scottish Parliament Health and Social Care Committee report in 2001 argued that sufferers should receive financial support, but largely rejected the idea of compensation:
‘100. Should this assistance that we advocate be described as compensation? “Compensation” implies negligence or fault, and on the (admittedly limited) basis of the evidence we considered, we do not think that this has been established. In the end, what matters most, in our view, is not what this assistance is called. What does matter is that it makes a clear, practical difference, and that it is delivered promptly. We would like to see a scheme established within twelve months’.
Compensation as an issue of intergovernmental relations (2003-)
It has been reported in late January that differences in legal advice to the UK Government and the Scottish Executive over the latter’s proposal to make ex gratia payments to Hepatitis C sufferers, whose condition was caused by contaminated blood, may have to be resolved ultimately by the Judicial Committee of the Privy Council. Two difficulties appear to be relevant, one of which (similar to earlier arguments over free personal care) involves possible clawback through the (reserved) social security system of some of the payments made by the Executive. The other relates to the more general question of whether the Executive actually has the power to make such payments. This appears to be a reference to Head F (social security) of the list of reserved matters in schedule 5 of the Scotland Act, which, in its interpretation provisions, may exclude such payments from the Executive’s devolved competence or the Parliament’s legislative competence”
Cairney (2006: 433) relates compensation to disputes between the UK and Scottish governments:
“This imbalance of power is apparent when disputes rise to the surface. The most high profile policy of the first Scottish Parliament session (1999–2003) was the decision in Scotland to depart from the UK line and implement the recommendations of the Sutherland Report on ‘free’ personal care for the elderly. … if the UK government had been sympathetic to the policy a solution would have been found, but general Whitehall indifference to Scotland had turned to specific hostility (particularly since UK ministers failed to persuade their Scottish counterparts to maintain a UK line). This approach was also taken with the issue of Hepatitis C compensation in Scotland, with the Department of Work and Pensions threatening to reduce benefit payments to those in receipt of Scottish Executive compensation (Lodge, 2003 reproduced below). This case was taken further, with Whitehall delaying Scottish payments on the basis of competence (health devolved, but compensation for injury and illness reserved) until it came up with a UK-wide scheme to be implemented in Scotland (Anon., 2004a)”
“Hepatitis C became a cause of relative tension, with the UK Government apparently willing to challenge the Scottish Executive’s right to provide compensation (payments related to injury and illness are reserved), until it came up with a UK-wide compensation scheme (with which Scottish ministers were less happy) (Winetrobe, February 2003: 39–40; February 2004: 42; May 2004: Cairney, 2006: 433; January 2007: 83). The Scottish Executive and UK Government also faced calls for a public inquiry into Hep C in 2006 (Cairney, September 2006: 75). The Scottish Government oversaw its own inquiry on Hep C, partly to put pressure on the UK Government to follow suit (Cairney, May 2008: 87; May 2009: 58)”
“The dispute between the UK government and the Scottish Executive, over the decision by the Executive to provide compensation to anyone who contracted Hepatitis C on the NHS in the 1970s and 1980s as a result of contaminated blood, has continued this quarter. The Scottish Health Minister, Malcolm Chisholm, announced proposals for ex gratia payments in January 2003, but has had to concede that no payments will be made until the Scottish Executive resolves the issue with Westminster. The dispute centres on whether or not the Department for Work and Pensions will try and ‘clawback’ the money used by the Executive in compensation through the social security system. There is also a debate over whether the Executive actually has the power to make such payments.
In what many in Scotland have interpreted as a snub to the Scottish Parliament, Andrew Smith, the Secretary of State for Work and Pensions, has refused to appear before the Health Committee, which had invited him to give evidence on the issue.
The SNP have been keen to raise the issue at Westminster. On 21 May, Annabelle Ewing quizzed the Prime Minister on why no compensation had been made during questions to the Prime Minister.
Annabelle Ewing (SNP – Perth): The Prime Minister will be aware that the Scottish Parliament agreed at the beginning of this year to pay compensation to hepatitis C sufferers in Scotland who contracted the disease through contaminated NHS blood products. However, not a penny piece has yet been paid, as a result of dithering by Westminster over jurisdiction. Can I inject a sense of urgency into the debate and ask the Prime Minister to confirm today that Westminster will not frustrate the will of the Scottish Parliament to pay compensation under exemption from the benefits clawback regulations? Surely the Prime Minister would agree that the people involved have already waited far too long for justice.
The Prime Minister: I am aware of the Scottish Executive’s decision to pay compensation to hepatitis C sufferers. I am not aware of the other particular problem to which the hon. Lady has just drawn attention. I shall look into it, and write to her about it.
Annabelle Ewing also raised the issue on 20 May at Scotland Office questions in which Liddell suggests that a decision will be made after the elections in Scotland.
Annabelle Ewing : Surely the key issue is whether she will fight for the right of the Scottish Parliament to pay compensation and for a 100 per cent exemption from the benefit clawback rules. If she will not do that, will she explain to hepatitis C sufferers in Scotland why on earth Scottish taxpayers are paying £7 million for the running costs of her office?
Mrs. Liddell: There are serious legal and policy-based issues in relation to hepatitis C. There have been extensive discussions between the Scottish Executive and the Department for Work and Pensions, not least on whether payments should be taken into account as capital or income when someone claims income-related benefits. Those discussions could not continue because of the Scottish Parliament elections. As soon as the Minister for Health and Community Care is in place in the Scottish Parliament, those discussions will continue”
This post by Sean Kippin introduces chapter 9 of Politics and Policy Making in the UK by Paul Cairney and Sean Kippin.Key terms to remember include:
Deficit: the amount to borrow when annual government spending is higher than income.
Debt: the overall amount of government borrowing (from multiple deficits).
Recession: a sustained drop in economic activity. Often defined as a reduction in gross domestic product (GDP) over two successive financial quarters.
From 1979 a ‘post-war consensus’ to pursue ‘Keynesian’ policies gave way to a ‘neoliberal’ approach which emphasised state withdrawal and market forces. This reduced the state’s control of its own economic policy, and left it subject to international forces. The response of successive UK governments to the financial crisis (which began in 2008) demonstrates how policymakers define and attempt to solve problems, the barriers they face when trying to enact their agendas, and the profound social consequences of their decisions.
Defining and solving the crisis
The global financial crisis of 2007-8 included the collapse of major banks in countries such as the US and UK. The UK was particularly vulnerable since its economy depends disproportionately on a large financial sector. The UK government sought to reinject financial sector ‘liquidity’ (access to cash or the means to convert assets to cash), since a failure to do so would risk economic collapse and terrifying social consequences. Its action took the form of enormous ‘bailouts’ to failing banks, including taking part-ownership of some. Such measures were controversial, as they seemed to let the banks off the hook for their risky lending practices and lack of prudence in managing their customers’ finances.
This immediate banking crisis created an economic crisis marked by recession and low growth. The response was to use mildly Keynesian economic policies to engage in counter-cyclical public spending to trigger economic growth, in the form of a ‘fiscal stimulus’. The combination of high spending and low growth generated attention to the issue of higher debts and deficits, with the Conservative Party benefiting from the issue politically and emerging as the largest party in the House of Commons following the 2010 General Election (then forming a Coalition government with the Liberal Democrats). Crucially, it gave them an opportunity to pursue longstanding neoliberal ideological goals.
The Coalition placed responsibility for crisis at the former Labour government’s door by claiming that they had ‘spent too much and ‘failed to fix the roof while the sun was shining’. This new problem definition was influential, reinforced by the unfolding Eurozone crisis, and triggered a shift to austerity whereby the Coalition pledged to eliminate the fiscal deficit within a single, five year parliamentary term. The Coalition related these issues to broader debates about the appropriate size and role of the state, the need for public sector reform, and the balance between tax rises and spending cuts which are socially just and economically viable.
Is UK economic policy within the Government’s control?
Economic policy has a strong international dimension, due to the centrality of international markets, the effects of currency fluctuations, and the interdependencies of globalised economic and financial systems. The UK government also handed power to an independent Bank of England from 1997 onwards, which sets interest rates and controls other elements of monetary policy (Chapter 4). The devolved executives also oversee important economic functions.
Conservative and Labour UK governments have supported neoliberal policies such as deregulation. Many have argued that such a hands-off approach helps to explain the severity of a global economic crisis as experienced in the UK.
While the outcomes of economic policy may be out of reach of UK governments, they have more influence over crisis narratives. For example, the Coalition government used a persuasive narrative to justify austerity, consisting of the following components:
Excessive debt is dangerous.
Britain is broke.
Austerity is a necessary evil.
Big government is bad government.
Welfare is like a drug, and government action should not encourage dependence.
Reform government to reward strivers and punish skivers.
We need to fix Labour’s mess quickly.
While the narrative was successful, UK policies were less so. Indeed, these policy choices were highly contested in relation to the following issues. First, UK debt levels were high, but affordable due to low interest rates. Second, the notion that the country had ‘run out of money’ was misleading and based on an inaccurate ‘domestic household‘ analogy. Third, despite the claims of the Coalition’s leading figures, there were alternatives to its approach. Fourth, a key element of austerity – that state intervention ‘crowded out’ the private sector and thus economic growth – is rather controversial. Fifth, it drew upon misleading claims about ‘welfare dependency‘ and a false distinction between in and out of work poverty.
Did the Government deliver austerity? And what were the consequences of its efforts?
The substance of the government’s austerity drive was spending cuts, tax changes, public sector reforms, and even a hike in English university fees (despite Liberal Democrat promises to the contrary).
The government cut spending heavily in some areas, such as local government and welfare, but not in others, such as money spent on old age pensioners and the NHS. It was more successful in projecting austerity than achieving its fundamental goals. Austerity harmed economic growth, and triggered a recession. Recession prompted a relaxation of spending cuts and even an intervention from the IMF. Public spending rose during this period, but fell as a proportion of GDP:
Other reforms, such as Big Society, and gimmicks like the ‘one in, two out’ rule for regulation didn’t amount to much.
The social consequences of austerity were severe, and felt unequally
Women received a ‘triple whammy‘ of cuts to benefits, and increase in employment, and the retrenchment of vital public services
The Department for Communities and Local Government was the hardest hit by cuts, which translated into particularly severe local budget cuts to large urban centres in the North of England, while ‘middle England’ received less harsh cuts, exacerbating existing regional inequalities.
In other words, the Coalition’s response to the economic crisis included policies which created social harms, backed by a top-down uncompromising language. If so, can we envisage more inclusive means of policymaking? Many ideas have been proposed:
– Constitutional reform, such as through greater devolution or electoral reform might help to include a greater breadth of perspectives in policymaking.
– ‘Co-production’ with service users and other citizens
– Deliberative democracy, to assemble a representative body of people engaged in a finding common ground and reaching decisions, could foster participation in and legitimacy for policy decisions
– Community wealth building to use ‘anchor institutions’ and member owned businesses to ensure wealth generated locally is kept there
Many of these agendas have been proposed and rejected. Others show less potential for transformation than their advocates might suggest. Some may some appealing, but lose support should they propose too-radical change.
Conclusion
This story of post-crisis economic policy connects strongly to the Westminster story. Politicians responded to crises by projecting strong control of the situation and of acting decisively to make hard decisions on banking, then economic crisis, then debts and deficits. However, it also confirms elements of the complex government story: policies did not have their desired effects, often leading to a course change. Public sector reforms demonstrate the usual mixture of eye-catching presentation and low impact. Austerity was ultimately more useful as a dramatic government story than a way of controlling economic policy and achieving goals on debts and deficits. A government can appear to deliver on its promises, but not getting what it wants, while causing damage along the way.
This chapter describes climate change as the ultimate ‘wicked’ problem, so let’s make sure we know what that means.Think of references to ‘wicked’ as Rittel and Webber’s rejection of ‘rationalist’ understandings of policy problems. Rather, wicked problems:
Defy simple definition and understanding. Indeed, the definition and alleged cause is contested.
The cause of this problem may actually be a symptom of another problem, or too complex to be compared to problems addressed successfully in the past.
It is impossible to know if all solutions have been identified, or if a problem is solved.
Trial and error is difficult, since errors have major social consequences
You might think – reasonably – that all policy problems discussed in this book are ‘wicked’, but are they ‘super wicked’?! Levin et al identify 4 additional properties that sum up super wicked problems like climate change:
‘Time is running out.’ The problem becomes more acute when solutions are not found.
‘Those seeking to end the problem are also causing it.’ Countries like the UK help to lead the climate change agenda, but are major contributors of emissions.
‘No central authority.’ There are global policy agreements to tackle climate change, but each government is responsible for its own implementation.
‘Policies discount the future irrationally.’ Actors place too little value on policies with long-term benefits and too much on short- term costs.
Climate change also sums up complex government themes (Chapter 3), since it is an existential crisis that has not been addressed adequately by current policies, and it exemplifies the gap between what is required to address the problem and what actually happens.
The requirement is for continuously high policy-maker attention, and for governments to collaborate: with each other, to connect domestic and global policy agendas; within government, to join up policy across many sectors; and, with non-governmental actors, to harness stakeholder ideas and connect government policy to the behaviour of businesses.
Yet, governments are slow to pay (fleeting) attention. They make useful references to energy, transport, and food system transformation, and frequent references to collaborative or integrated policymaking inside and outside of government, but with limited effects.
How can we explore these issues with our 3 lenses?
Policy analysis: how to address the policy problem
We use 5-step policy analysis to understand the problem through the eyes of policymakers:
Step 1. How could governments define climate change as a policy problem? We see contestation to give the problem a name and assign authority to organisations (like the IPCC) to describe its size, urgency, and cause.
Step 2. Identifying feasible solutions. While the IPCC focuses mostly on technical feasibility, the UNFCCC focuses on limited political feasibility. For example, maybe the Paris Agreement represents a profoundly useful ‘Legally binding international treaty on climate change’, or maybe it allows countries to signal commitments without follow-through.
Steps 3 and 4: Using values and goals to compare solutions, and predicting the outcomes of solutions. For example, the Stern Review produced a cost benefit case to demonstrate that, in the long run, it would be better for global GDP to address climate change effectively.
Step 5: Making recommendations. Policy analysis texts advise that recommendations should be simple and punchy to make the problem seem solvable and the solution seem feasible. Yet, environmental defies simple analysis, and a list of technically and politically feasible solutions is generally absent from international agreements.
Policy studies: What exactly is UK environmental policy?
Environmental policy can relate to (1) natural resources (water, air, forestry, land, coast), waste and pollution, climate change, and ecosystems, and (2) relate strongly to policies on energy, transport, food/ agriculture. This spread raises immediate issues:
It is difficult to map policymaking if everything is so connected and multi-level (EU, UK, devolved, local) and multi-sectoral (energy, transport, food, climate, environment).
It is difficult to coordinate policymaking, such as to establish a unit without enough power or ‘mainstream’ a climate policy aim across sectors with other bigger priorities.
How did the UK and devolved governments respond to climate change?
We describe limited then sporadic policymaker attention, followed by high EU activity from the 1980s, and some UK measures from the late 1990s to use taxes and regulations to address climate change. There was a brief but strong ‘competitive consensus’ from 2006, in which the governing party (led by Tony Blair) and opposition party (David Cameron) competed to establish their green credentials. This dynamic reinforced the motive and opportunity of Labour ministers to propose rapid and radical changes to policy
Policy changes included:
The Climate Change Act 2008 to increase the government’s emissions reduction targets and give them statutory weight
Policies to incentivise renewable energy and encourage more efficient homes and electric vehicles.
Policymaking changes included introducing the Office for Climate Change to coordinate responses (2006), independent Committee on Climate Change (CCC) to report on UK progress, and Department for Energy and Climate Change (DECC) to lead policies to meet targets (2008).
Still, climate change was not a top priority for long, and the coalition government from 2010 was keener to support policies to reverse recession and prompt economic growth (e.g. supporting oil and gas).
There was resurgent interest by 2019, to amend the Climate Change Act to set a ‘net zero’ target by 2050 (the amount of new GHGs entering the atmosphere is matched by the removal of GHGs) and establish UK and devolved government strategies to that end. Still, we are witnessing the gap between climate change aims versus outcomes, in which governments make big long term commitments, achieve the easy short term stuff, do things that undermine these long term commitments, and pass the rest to their successors.
Case studies: energy, transport, food
Chapter 8 examines this relationship between high ambition and limited progress:
UK renewables policy is a partial success story, featuring a long term shift from coal to renewables (especially Scotland), often backed by government economic incentives to invest in renewables. At the same time, UK governments support fossil fuel extraction and use, especially when faced with periods of energy insecurity and high global energy costs.
UK transport policy exhibits a post-war legacy of unsustainable policies (e.g. to support roads and car use). Reforms are difficult and thankless (e.g. to promote public transport), governments juggle multiple aims (transport, economy, climate), many remain unfulfilled, and integration and coherence are elusive.
Postwar food systems are unsustainable. Brexit perhaps offered the opportunity to reform more quickly than in the EU, but we are yet to see the fruits of such initiatives.
Critical policy analysis: who matters to policy makers?
Chapter 8 describes the pursuit of a ‘just transition’ from high to low carbon energy systems. Here, climate justice can describe: being seen as a legitimate contributor of relevant knowledge (recognitional), fair rules and processes to make decisions (procedural), and the fair distribution of costs and benefits associated with climate change and policy (distributional).
At the international level, issues include: the UK causes a disproportionate share of the problem, but does not bear proportionate costs, so climate change is a foreign policy, trade, and international development as well as an environmental issue. At the domestic level, problems such as fuel poverty endure despite the promotion of UK and devolved strategies, and there is contestation to determine who is in greatest need, who should bear the burden of costs (people, business, government), and if energy justice is a human rights issue.
Conclusion
Both of our policymaking stories signal bad news for the environment. The Westminster story could be harnessed to generate support for rapid and radical policy change, driven by a centralised focus on addressing an urgent problem. Rather, we see bursts of attention and limited follow-through. The complex government story describes the absence of single central government control over policy outcomes. Some is by choice, such as to privatise energy then minimise regulation. Some is by necessity, in which policymakers struggle to understand systems far less control them. Central governments often exacerbate this confusion by fudging their stories of policymaking – we are in control (the Westminster story) and we are not in control (the complex government story) – to project a sense of governing competence but avoid full responsibility for policy outcomes. The result is that UK (and devolved) governments have described maximally their ambitions to deal with climate change, but minimally how they will achieve them.
This chapter relates UK state transformation (Chapter 4) to the Westminster and complex government stories explained in Chapter 3.
We ask four key questions.
Q1. What was the style of policy making during transformation?
Did governments push new policies from the top-down, in line with the Westminster story? Thatcherism stories played up to this idea:
Using the ‘there is no alternative’ language. Don’t waste time on consultation when you know you need to be radical
Basing an image of governing competence on making strong decisions from the top-down
Bashing unions, and brooking no opposition from vested interests.
The complex government story warns against the assumption that this style was ‘normal’ rather than based on high profile examples. In a wider policymaking environment, over which they have limited control, policymakers seek a range of styles. Chapters 2 and 3 use the concept of policy communities to make this point:
Ministers have to ignore most issues, and delegate most policymaking to civil servants
Civil servants form relationships with groups
Civil servants see clear political benefits to consultation, to foster stakeholder ownership and policy legitimacy
Groups recognize the benefit of insider strategies (following the ‘rules of the game’ to maintain good access).
Still, long-term transformation had an impact on policymaking: the ‘normal’ policy style today is not the same as in the 1970s. Examples include:
Many groups – such as trade unions – never returned to the status that they enjoyed in previous eras.
Many policies – such as new public management (NPM) reforms (Chapter 4) – were opposed vociferously in the past, but now taken for granted.
These reforms changed the role of the civil service, which became less central to policy making (Chapter 4).
Both governing parties have exploited crises to make ‘tough choices’ backed by the ‘government knows best’ narrative.
Richardson describes a new normal style: making announcements then consulting on delivery. We describe a mix of co-existing styles: (1) high profile imposition, and (2) routine low attention issues and consultation.
We then describe the face value contrast between UK (majoritarian) and devolved (consensus) policy styles, but warn against the assumption of a contrast based on high-profile examples. Instead, ask yourself: what is the mix of styles across the political system (see Boxes 3.2 and 5.1)?
Q2. Did policy change incrementally or in radical bursts?
Chapter 4 describes long periods of policy continuity, but major shifts associated with some periods (the mid-1940s and late-1970s). In some cases, a new government signalled an era-defining shift in direction. In many others, policy slowed down or accelerated. The Westminster story has some value, to describe periods of radical change directed from the centre, but only when situated in a wider context to identify the rarity and effect of these changes.
These dynamics are not summed up well by ‘incrementalism’ (Chapter 2). If we treat incrementalism as a strategy, we exaggerate the coherence of steps towards an endgame. If we treat it as a description of policy change, we struggle to explain key periods that do not fit the pattern. Instead, we need to account for
Long periods of policymaking stability followed by a burst of instability (or vice versa).
Long periods of policy continuity followed by a shift in policy direction in relation to one problem. Or, the combination of many minor policy changes and a small number of major changes.
Punctuated equilibrium theory helps to explain these dynamics. See the separate blog posts for the general background:
Here, we focus on the contested idea that policy changed profoundly during Thatcher’s first term. Hall describes ‘third order’ change: rare, radical shifts in policy (1) prompted by failure to explain the problem or address it, (2) prompting the replacement of one paradigm (world view) and approach with another. Oliver and Pemberton argue that policy change was less of a clean break, and more about the accumulation of change.
There are many phrases that try to sum up this gradual but profound change to policy and institutions. In Chapter 5, we relate that idea to this wider discussion of paradigm coherence (State transformation: trial and error, not a grand plan). Examples include:
There was no grand privatisation plan. It took off when it proved feasible and popular.
There was initial reticence over challenging unions under Thatcher (similar moves had failed under Heath).
Public sector reform was a mish-mash of changes, not a grand New Public Management plan.
In other words, we warn against assuming a grand coherent state transformation plan, and show that it is tricky to know if we witnessed a few radical steps or a collection of less radical measures adding up (eventually) to transformation. The difference might seem ‘academic’, but is actually more important to governments wondering if they can deliver on radical intentions.
Q3. What was the impact of state transformation on central government?
We describe ministers addressing the unmanageability of government, either to reassert central control or jettison the parts of government that defy it. Have these reforms reduced or exacerbated the limits to central control?
There is a lot of academic uncertainty and contestation on this point.
One interpretation is consistent with the Westminster story: reforms contributed to a ‘rejuvenated’ and ‘lean’ state, with ministers able to focus on core tasks without having to manage peripheral functions. They can make strategic decisions, create rules and regulations – backed by funding, inspection and performance management – to ensure that their aims are carried out by others, and minimise the powers of other public bodies.
Another interpretation is that the UK government exacerbated its own ‘governance problem’ (the gap between a story of central control and what central governments can actually do). A collection of reforms fragmented the public landscape and exacerbated a sense that no one is in control. There is a never-ending and dispiriting cycle of such reforms, where a lack of central control prompts futile attempts at centralisation.
Similarly, there is a lot of government uncertainty. Conservative and Labour governments have: bemoaned some aspect of limited central control; reformed to solve the problem; found that many reforms just changed the problem; and had to project the sense of being in control regardless (Chapter 3).
Q4: How do these UK developments relate to the wider world?
‘Globalisation’ suggests that national governments do not simply manage their own affairs. Their high profile aims depend on choices made by other governments, international organisations and non-governmental actors such as multinational corporations.
For example, economic policies relate to:
international financial markets that influence the value of a country’s currency
the technology that allows a global trade in goods and services
the power of multinational corporations, seeking the most favourable taxation, subsidy and regulatory systems from countries competing for their business
the migration of people seeking work in a country
the power of international organisations such as the IMF to set strict conditions on a government’s policies – to reduce state intervention and reform public services – in exchange for financial assistance (as with Labour in the late 1970s)
For example, ‘race to the bottom’ describes many countries pursuing ‘neoliberal reforms’ to please corporations by (1) minimising costly regulations, (2) reducing spending to reduce demand for taxation, (3) privatizing.
We describe a UK variant of neoliberal state transformation.
The Westminster story helps to interpret key Labour (1945) and Conservative (1979) governments setting a radical new policy direction. The Thatcher period drew on this story to narrate radical change, and promised a lean state less prone to ungovernability.
The Complex government story helps to narrate an uneven direction of policy, ad hoc reforms with limited impacts, path dependence and policy inheritance, and an incoherent state.
These long-term questions, of what happened and why, are crucial to the analysis of shorter term bursts of activity in chapters 6-11.
State transformation describes a collection of major changes to policy and policymaking from the ‘post-war settlement’ towards ‘neoliberal reforms’ (towards a smaller state and less state intervention). There were many ‘neoliberal’ reforms to UK policy, policymaking, and delivery functions from the election of a Thatcher-led Conservative government from 1979. However, we are not really describing a coherent and wholesale shift from one model of state intervention to another. Further, the election of a different party did not necessarily prompt a wholesale shift of approach.
What was the post-war consensus?
Consensus describes the maintenance of a similar approach to policy and policymaking throughout multiple changes of Labour and Conservative government (from 1945). This approach is characterised by higher state intervention to address policy problems. It includes:
A Keynesian approach to economic policy (high state intervention via fiscal policies).
An expanded welfare state, withnew entitlements to social security (including pension, unemployment and child benefits), access to free public services such as healthcare and education, and subsidized social housing.
A large industrial state, with high state ownership of industry and public utilities.
The funding and direct delivery of public services.
What were neoliberal reforms?
Neoliberal can mean the preference for: individual rather than state responsibility (e.g. for improving your health), market rather than state action (e.g. to promote economic growth), and economic growth as the primary aim. As such, reforms would include:
The rejection of Keynesian intervention, based on belief that state intervention harms market forces, in favour of controlling inflation via monetary measures.
Reduced policy commitments in relation to full employment and the welfare state, and being prepared to trade higher unemployment for low inflation. For example, the idea may be to seek a ‘natural rate of unemployment’, or the lowest level of unemployment that does not cause excessive inflation via inflationary wage demands, exacerbated by the negotiating power of trade unions, and too- high unemployment benefits.
The privatisation of industry and reform of public services.
Economic Policy: From Keynesianism To Neoliberalism?
Chapter 4 describes a series of broad phases of activity, including:
1940s and 1950s: UK government policy changes consistent with Keynesian thought. For example, high taxation and spending to manage demand and seek full employment.
1960s: making state intervention work by modifying a Keynesian approach. For example, defending a Keynesian approach but modifying action to address unexpected problems (e.g. lower than expected growth, and a currency crisis)
1970s: a series of crises. They included the Conservative government (1970-74) seeking in vain to ‘roll back the state’, then a Labour government (1974–1979) facing rising inflation and unemployment, and a reduction in the value of sterling. The government’s need to borrow heavily, to finance major spending deficits, prompted initial attempts to reduce public expenditure.
1979–1997: a rejection of Keynesianism?Peter Hall describes a ‘paradigm change’ from Keynesianism to monetarism in the early 1980s, while Oliver and Pemberton describe longer term change towards neoliberal approaches.
1997 onwards: a mix of ‘neoliberal’ aims and new Keynesian’ policies. The New Labour government (1997-2010) sought to project an image of economic competence based on fiscal prudence (keeping government debt to 40% of GDP), granting independence to the Bank of England, and minimizing regulation of ‘the City’ (financial institutions).
Then came the global financial crisis, high state intervention, then ‘austerity’ (Chapter 9). Overall, we describe from 1979 an often-confusing mix of low-state intentions and unwanted high state action during crisis.
The story of employment policy is less confusing: from 1980 there has been a succession of Employment Acts to restrict the power of trades unions, based initially on Thatcher government antipathy to unions and consultation with interest groups (chapter 5), but maintained under Labour and accelerated by Conservative governments. The ability of trades unions to organize and call strike action has been reduced profoundly.
Privatisation and new public management
There has been a profound shift from a UK industrial state. For example, in 1950, the nationalized industries – water, coal, electricity, steel, gas, oil, rail, telecommunications and postal delivery – employed 2.3 million people. In 1980 they employed 1.8 million. By 1997: 0.24 million. UK governments sold £74 billion of state assets from 1979-1997 and £8 billion since then (2020 prices).
Thatcher governments also encouraged the mass sale of social housing. The 1980 Housing Act introduced a renter’s ‘right to buy’ their council house (and a discount based on years of renting). From 1980-2003, 2.8 million homes were sold. To some extent, this obligation for councils was part of a wider challenge to local authorities, which included the ill-fated poll tax.
Privatisation also extended to:
deregulating services (e.g. buses)
obliging the private delivery of public services (e.g. making public bodies like councils ‘contract out’ some services)
using private investment for capital projects (e.g. to fund investment in roads, bridges, hospitals, schools)
reducing subsidies or increasing charges for services (e.g. for prescriptions, opticians, higher education tuition).
New public management reforms involve the application of private sector ideas or methods to the public sector. Examples include:
NHS reforms to introduce an ‘internal market’
Education (schools) reforms in England to foster ‘school choice’, shift from comprehensive schooling, and shift from local authority control.
Civil service reforms, to reduce their number, recruit from outside, and separate policy and delivery (in Executive Agencies). Governments have also sought to establish new policy advisory systems (with more involvement from consultancy and think tanks)
Measures of state retrenchment or transformation
It is not always straightforward to demonstrate state transformation. For example, state spending as a proportion of GDP was 45% in 1988, which was lower than 1982 (54%) but higher than the mid-1950s (then it rose heavily under New Labour before ‘austerity’ from 2010 – Chapter 9). Still, the industrial state has vanished, and the role of the state in public service delivery has transformed (see Chapter 4 for examples). ‘Neoliberal’ also extends to a reluctance to foster ‘nanny state’ intervention.
The impact of devolution on state intervention
One the one hand, political devolution in 1999 represents the further transformation of the state towards multi-level policymaking. On the other hand, devolved governments are usually less keen on neoliberal reforms (although it is difficult to present a complete picture in Northern Ireland, since its Assembly was suspended in 2000, 2002–2007 and 2017–2020, and in flux from 2022-4). Examples include:
Healthcare. The Scottish and Welsh governments sought to remove or slow UK reforms. All 3 governments phased out prescription charges.
Schools. The Scottish and Welsh governments prefer comprehensive schooling. All 3 are less keen than the UK on ‘league tables’ of school performance.
Local government. The Scottish and Welsh governments foster better central-local relations, and more trust in public bodies to deliver services.
Overall, there has been a transformation of the UK state
It moved from a ‘postwar consensus’, built on the belief that governments could and should intervene to benefit the UK population by delivering employment, education, healthcare, housing and social security. It moved towards ‘neoliberalism’, built on the belief that state intervention undermines the market and that individuals should take responsibility for their welfare. The size of the industrial state fell dramatically. The UK government is less committed to the ‘old’ Keynesian measures to tax and spend to manage demand in the economy. Tax- funded public services remain, but the state is much less likely to deliver them directly. Multiple reforms have changed how the civil service and policy advisory systems operate.
Parties made a difference to this transformation. Labour introduced the policies associated with the post- war consensus, and the Conservatives pursued a commitment to neoliberalism. However, parties also inherited the commitments of their predecessors, accepting or accelerating policies of the past. Most elements of state transformation are here to stay, regardless of party.
See also Chapter 5 on how we can describe and explain the transformation.
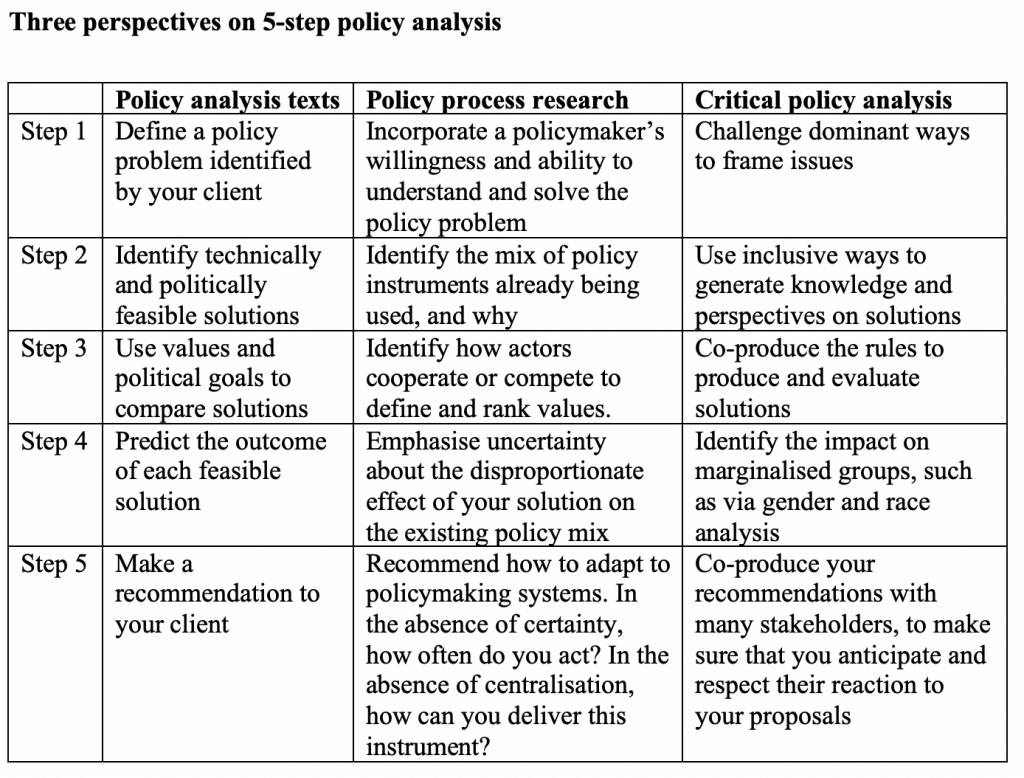
Chapter 2 outlines the structure for UK policy case study analysis, comparing three perspectives: policy analysis, policy studies, and critical policy analysis.
This post summarises Chapter 2 but also signposts a wide range of additional resources on Cairney’s website to aid the study of UK policymaking, including:
The 750 page which includes a separate book, blog post, and podcast series on the 3 perspectives introduced here.
The 1000 and 500 pages which include a separate book, blog post, and podcast series on concepts and theories in policy studies.
Key examples of useful preparatory reading include:
5-Step guides break the policy analysis task into key requirements:
Define a policy problem identified by your client.
Problem definition requires analysts to gather sufficient data on its severity, urgency, cause, and our ability to solve it. Problem definition is a political process involving actors exercising power – such as through argumentation – to make sure that policymakers see a problem from a particular perspective.
2. Identify technically and politically feasible solutions.
Policy instruments have to work as intended if implemented (technical feasibility) and be acceptable to enough powerful people (political feasibility).
3. Use value-based criteria and political goals to compare solutions.
For example, values include efficiency (the maximum output for the same input) and equity (fairness of process and outcome). Political goals include the desire to make policy changes without facing too much opposition or unpopularity.
4. Predict the outcome of each feasible solution.
In other words, find reasonable ways to signal what would happen if you made this policy change.
5. Make a recommendation to your client.
Perspective 2: Policy studies
We then relate these simple guides to messier reality. Policy studies provide a contrast between ideal-types (artificial models) and real world policymaking.
This is not an evidence based process in which there are clear and obvious technical solutions to social and economic problems. It is a political process to get attention, define problems, and get the solutions you want. Policymakers need information to reduce uncertainty, but rely on their beliefs and exercise power to reduce ambiguity.
2. It is not a simple process with clear analytical stages mapping onto policymaking stages. Rather, think of these stages as essential functions or requirements, not what really happens. Or, the policy process contains a spirograph of cycles.
There are many ways to conceptualise these aspects of real world policymaking, in which policymakers are dealing with bounded rationality and complexity:
Incrementalism as a pragmatic response: (a) only analyse a few feasible solutions, (b) only depart incrementally from the status quo.
Punctuated equilibrium theory suggests that policy change is actually hyper-incremental and radical, not simply incremental. Why? Attention to one problem means ignoring 99 others. As chapter 3 suggests, ignoring the 99 other issues actually means delegating to policy communities.
The Advocacy Coalition Framework describes people entering politics to turn their beliefs into policy, forming coalitions with like-minded people and competing with other coalitions.
What is the common link?
Policy analysis is not a rational or technical response to problems.
It is a political act, taking place in a policy process over which no one has full understanding or control.
This act produces one more instrument to add to the overall ‘policy mix’. What we call ‘policy’ is actually a collection of instruments that have accumulated over time, and it is difficult to know what an additional instrument will do.
We can represent these common concepts in an image that (1) is as simple looking as the policy cycle, but (2) hints at policymaking complexity across many different ‘centres’.
This image tells a story that contrasts with the ideal type of comprehensive rationality and the policy cycle.
Instead of one powerful centre, there are many.
Instead of producing rational, orderly and stable policy making, these centres combine to produce dynamics that can be stable or unstable, and outcomes that can lurch from continuity to change.
A political system’s ‘central government’ may be the most powerful centre, but it tends to be broken down into many smaller ‘policy communities’ (see Chapter 3).
Senior policy makers could intervene in any issue at any time, but the logical consequence is to ignore most other issues.
Perspective 3: Critical policy analysis
For our purposes, CPA performs three tasks:
It pushes back on the idea that policymaking is chaos with random outcomes. Maybe the policy process is complex, but it is still characterized by unequal access, power, and outcomes.
The overall value of 3 perspectives on the study of UK politics and policymaking
5 step guides encourage the analytical and technical skills to interrogate policy problems systematically.
Policy studies relate these analytical processes to real world policymaking. Put simply, analysis focuses on what we require from policy and policymaking to solve problems. Policy theories and concepts explain why these requirements are not met in reality.
Critical policy analysis reminds us that policy analysis is not a rational, technical, objective process. It is a political process with unequal recognition and contributions of policy relevant knowledge, unfair rules, and unequal outcomes.
We need all three perspectives to: (1) analyse the UK’s pressing problems, (2) identify barriers to action (in chapter 3, by contrasting Westminster and Complex government stories), and (3) identify and challenge the inequalities that endure in politics and policymaking.
It might seem like there is never a good time to read a book on contemporary policymaking in the UK. Politics moves too fast, and politicians come and go. Policymakers lurch from crisis to crisis without giving the impression that they understand policy problems or control the outcomes of their responses.
We anticipated this problem by focusing on case studies that are important to readers, because they (a) are contemporary, and (b) highlight themes that endure for years. For example, the cases include:
Covid-19, which dominated life from 2020 while raising longer-term issues about state intervention to boost population health and reduce inequalities.
Brexit, which dominated politics in the mid-2010s and raised longstanding issues about who should be responsible for UK policy.
Climate change, which represents an existential crisis receiving sporadic policymaker attention.
Austerity, the stated aim of the 2010 Coalition government and a reflection of long-term aims to reduce state intervention.
Inequalities and protest, which are enduring features of UK politics which attract fleeting attention during major events such as the ‘London riots’.
Foreign policy and war, including the Iraq War and its legacy on UK politics.
We identify three ever-present themes that help to understand these case studies.
Theme 1: Three complementary perspectives on the study of policymaking
Chapter 2 describes three ways to analyse the relationship between policy and policymaking in countries like the UK:
Policy analysis is a political act to identify important problems, generate feasible solutions, engage in trade-offs, estimate what will happen, and make recommendations or choices.
Policy studies describe and explain how policymaking actually works. If policy analysis is about what we require, policy theories identify the gap between requirement and reality. For example, we need policymakers to understand problems and be in control of delivering solutions. Yet, they must act despite uncertainty and contestation to define problems, and the link between their choices and outcomes is not clear.
Critical policy studies identify profound inequalities in social, economic, and political power and the outcomes that follow. Maybe policymaking systems defy control, but there are still patterns of inequalities that reflect the power of some and powerlessness of others.
Theme 2: Two essential perspectives on UK politics and policymaking
Chapter 3 relates these general perspectives to the specific UK context, with reference to two essential stories:
The Westminster story of how policy should be made. Elect a powerful government to translate a manifesto into outcomes. Then, if you know who is in charge, you know who to re-elect or replace. This story is part of a fixation with political parties and UK general elections elections, as if that’s all there is to politics.
Complex Government stories of how things work. Elect governments with limited knowledge of problems, operating in a complex system containing many different influences on policy and outcomes. In other words, the stuff that happens in between elections.
The first story is simple for all and aspirational for some. The second story is complicated, with lots of variants and less clear aspirations. We separate them analytically but, in practice. they combine to produce a confusing story of ministers performing the idea of being in charge (to seek reelection) but adapting to their limits (to try to get things done).
Theme 3. Long-term changes inform current discussions (Chapters 4 and 5)
Chapter 4 explains that the UK state has transformed since the 1970s, from:
Post-war consensus characterized by high state intervention, including Keynesian approaches to economic policy, an expansive welfare state, state ownership of public utilities, and government delivery of public services.
Neoliberal reforms characterized by reduced state intervention, including non-Keynesian approaches to economic policy, reduced welfare state entitlement, the privatization of public utilities, and contracting out the delivery of public services. Broadly speaking, ‘neoliberal’ describes a preference to (1) encourage individual and market rather than state solutions, and (2) prioritise economic growth over other policy aims).
Chapter 5 asks how we can describe and explain the transformation:
Was it secured via top-down imposition by a powerful central government?
Did it happen in a series of incremental steps or bursts of radical change? Was it part of a clear long term plan, or a patchwork of reforms?
Did it produce a leaner and more effective state, or exacerbate problems of low central government control?
Was state transformation specific to the UK or part of a global neoliberal trend?
This focus on three enduring themes provides a structure for case study analysis (Chapters 6-11). In each chapter, we use (1) three perspectives on policymaking to describe what is going on, (2) UK stories (Westminster and complexity) to interpret these developments, and (3) a long-term perspective to relate current problems to longstanding approaches. This approach helps us to understand and interpret new developments with reference to well established ideas.
UK politics always seems to be changing, with UK government ministers lurching from crisis to crisis. Still, we have ways to make sense of chaos.
First, we place the actions of UK governments and ministers in a wider context. Ministers clearly matter, but they are part of a complex policymaking environment over which they have limited knowledge and even less control. They make then delegate choices, and what happens next is beyond their control.
Indeed, when you consider the case studies in this book, can you think of many policy outcomes that ministers wanted to happen? For example, is this what they meant by getting Brexit done? Did they really do all they could to minimise the fallout from COVID-19? Are they solving the climate crisis? Did they retreat victoriously from Afghanistan and Iraq? Is the economy working in the way they planned?
Second, we place this study of UK policymaking in an even wider context, to harness insights from policy theories. They suggest that a focus on policy analysis at the ‘centre’ of policymaking is not entirely useful because this approach identifies what peoplerequireofpolicymaking, not what happens. We focus on how policymaking actually works. We do so through a critical lens: analysing who has the power to define and address policy problems, which social groups they favour and marginalise, and who wins and loses from policy outcomes. In that context, things are always changing but stay the same. New policymakers emerge, but face the same constraints. New issues emerge, but inequalities endure.
These insights help us to engage with the following phrase that often seems to sum up British politics.
It is common to bemoan a lack of competence and trustworthiness of British policymakers. They don’t know what they are doing, and few trust them to get the results they promise. If so, would a change of government bring in better politicians? This idea forms part of the Westminster story in which a small number of senior ministers are in control. This story asserts how politics should work: if UK government ministers are in charge, we can hold them to account for policy. If they do badly, they can be replaced. It does not describe how British politics actually works.
Policy research provides a more useful story: the state is too large to be controlled by a small number of powerful individuals, and the complexity of policy problems and processes ensures that they are beyond anyone’s full understanding. These limits apply to policymakers regardless of their competence, sincerity, or trustworthiness, and we do a disservice to democracy if we ignore them in favour of simplistic stories of bad politicians.
That said, the Westminster story remains important. UK government ministers might not be in control, but they remain powerful and can still do damage. Further, the Westminster story still helps to structure government and fuel political debate. Think of British politics as a confusing conflation of two different stories: of the concentration and diffusion of policymaking power. UK government ministers have to juggle these images to project an image of governing competence based on the sense that they are in control and worthy of re-election. While no group can control policy outcomes, it would be wrong to ignore regular patterns of social, economic, and political life. Some people win, many people lose, and these patterns result from unequal access to resources. We therefore seek the right balance between accepting policymaking complexity and the limits to policymaker control and believing that well designed policies, taken forward by key people and organisations, can improve people’s lives. This approach requires us to reject superficial stories of UK politics and try to understand and engage with policymaking in the real world.
This post by Sean Kippin introduces chapter 7 of Politics and Policy Making in the UK by Paul Cairney and Sean Kippin. It examines Brexit, which is a portmanteau combining Britain and exit from membership of the European Union. The Brexit referendum ballot wording was ‘Should the United Kingdom remain a member of the European Union or leave the European Union?’ and people could vote to ‘Remain a member of the European Union’ or ‘Leave the European Union’.
Photo (9.12.20) of UK Prime Minister Boris Johnson (left) and President of the European Commission, Ursula von der Leyen (right) (Source)
The UK’s decision to leave the European Union (EU) in January 2020 was a major constitutional change. A June 2016 referendum delivered a narrow but decisive victory for ‘Leave’ over ‘Remain’’ (52% to 48%).
The Leave slogan ‘take back control’ drew on the Westminster Story (Chapter 3) to present EU membership as incompatible with British democracy and sovereignty. However, turning Brexit into policy reality in the intervening years illustrated the lack of control that UK policymakers actually have over decisions, outcomes, and consequences.
In Chapter 7, we relate Brexit to three perspectives: as the symbol of a policy problem (policy analysis), policymaking problem (policy studies), and problem of social and economic inequalities (critical policy analysis).
Policy analysis: how did policymakers approach Brexit?
We describe the referendum as a poor solution to an ill-defined problem. For example, former Prime Minster David Cameron had treated the referendum as a means of placating his party and the Eurosceptic media following his failure to renegotiate the UK’s terms of membership (Cameron then resigned after the vote). For others, Brexit was the alleged solution to a poor economy or low control over immigration, or the campaign was part of a ‘populist’ approach to relate EU membership to control by out of touch political elites.
5 step analysis helps to analyse Brexit as a policy problem and help to identify the problems faced by new Prime Minister Theresa May. First, actors defined Brexit as a problem in different ways: they debated over when to trigger Article 50, what powers the government had to enact Brexit, the UK Parliament’s role, and which issues to pursue in preliminary negotiations.
Second, policy actors identified very different feasible solutions, such as:
‘Soft Brexit’, leaving the EU but retaining economic union by remaining in either or both of the Single Market and Customs Union.
‘Hard Brexit’, leaving EU institutions, but coming to various bilateral agreements over areas of mutual interest.
‘No deal Brexit’, leaving without any formalised arrangements (often treated as the ultimate bad outcome).
Some proposed different avenues to avoiding or ‘undoing’ Brexit, such as a confirmatory or second referendum (known by advocates as a ‘People’s Vote’).
Third and fourth, the main trade-offs between (and estimates of the effect of) the different solutions amounted to favouring sovereignty (i.e. control over trade and immigration policy), or maintaining economic union and a soft border between Northern Ireland and Ireland. Theresa May announced ‘red lines’ which closed off many possibilities. The status of Northern Ireland involved particularly contested trade-offs. Ultimately, political dynamics and feasibility issues ruled out many options, including soft Brexit and No Deal Brexit.
Fifth, the House of Commons failed to find a mutually acceptable way forward (including ruling out the ‘attractive fudge’ of the ‘Chequers Plan’). May resigned and was replaced by the Brexit campaigner Boris Johnson. Johnson called and won a General Election, then secured a similar deal to one considered by May (though Johnson’s government would keep Northern Ireland within the Single Market, to the consternation of Northern Ireland unionists). A ‘differentiated Brexit’ would ultimately take effect in 2020.
Policy studies: did Brexit change the UK’s ‘multi-level’ policymaking system?
Brexit exposed long-standing debates about the feasibility and fairness of different ways to govern. Debates on ‘multi-level governance’ explore whether there is an ‘optimal’ division of policymaking functions, such as in one authoritative centre or shared between different ‘territorial’ levels of government. Advocates of multi-level governance argue that the dispersion of power across different centres is more efficient and democratic than central state control, but these divisions relate more to the competing political demands to take or share power at the different levels, rather than a technocratic process of constitutional design.
There is some evidence that the UK government has become more centralised and majoritarian in approach, although the impact is difficult to measure. The main sectoral changes (Table 7.1 below) are in salient areas, such as immigration, where the UK has ended the ‘free movement of people’ (a key European freedom) and now operates a reformed trade regime (but has not really solved the problem of immigration described by prominent Leave campaigners). There have also been constitutional knock on effects, such as the adverse impact of the new UK internal market policy on devolved government autonomy (accentuated by high profile disputes, such as regarding the UK government’s veto of the Scottish Parliament Gender Recognition Reform (Scotland) Bill).
Critical Policy Analysis: Who is winning and losing due to Brexit?
The clear winners of the impacts of Brexit are hard to identify. So far, it is far easier to identify losses, and to note that those with more resources are far better placed to endure the hardship. According to some Leave campaigners, but not reality, some of the biggest beneficiaries of Brexit were to be a ‘left behind’ working class, centred in the deindustrialised ‘emblematic sites of revolt’ such as Sunderland. Rather, there have mostly been visible losses, such as among the minority ethnic groups, women, and disabled people who lost EU funding and important legal protections.
How does Brexit inform our Westminster and Complex Government stories?
The ‘take back control’ message embodies the Westminster story of centralised top-down control, but the Brexit process exposed the limits to that control. The Government endured years of delay and political setbacks, provoking multiple leadership crises which threatened the viability of Brexit and ended successive premierships. The process also exposed the limitations of the UK Parliament, which couldn’t find a solution to an ostensibly straightforward problem (outlined in detail by UK in a Changing Europe).
Brexit challenges one aspect of the complex government story by simplifying the multi-level policymaking system. However, policymaking complexity remains a necessity, reflecting bounded rationality and the inevitable delegation of policymaking to a large number and wide range of actors across the UK political system.
Take home messages
The Brexit referendum illustrated the strength of the ‘Westminster story’, when voters chose to ‘take back control’.
Brexit entailed years of delay and setbacks, political crises, threatening its viability. It illustrates the complexity of the policymaking process.
The post-Brexit system is relatively simplified, removing one ‘level’ of government, however complexity and delegation are a necessity rather than a choice.
Brexit created many losers, and few winners. Those with greater resources are generally better able to withstand the negative consequences.
The UK political system often seems confusing because commentators are juggling two stories of policymaking.
The first is the official account of how policy is, and should be, made: the Westminster story. It emphasises strong, responsible, policymaking by very few powerful minsters at the heart of government.
The second comes from accumulated wisdom from policy studies about how policy is really made: the complex government story. It emphasises profound limits to central government control and the existence of many ‘centres’.
In that context, our question for reflection is: if the official story is so inaccurate, why does it matter and endure?
Story 1.The Westminster story (or model)
This story begins with how policy should be made: you only know who to praise or blame if you know who is in charge. Democratic accountability requires strong and decisive government. The ‘British political tradition’ is of responsible government: doing what is right for the public (even if it is unpopular).
To that end, the Westminster model is backed by measures to ensure strong central government:
Representative democracy. Vote for people to act in your constituency’s interests.
A sovereign Parliament delegating power to a strong executive. Maintain strong government legitimised by an elected (and unelected) legislature.
Plurality elections and majority party control. Exaggerate support for the winning candidates, and biggest party, to concentrate power.
Unitary state. Maintain central government control across the UK.
Prime Minister and Cabinet Government. Vest overall decision-making in an executive committee filled with senior ministers and led by the most senior minister.
Individual Ministerial Responsibility. A senior minister is in complete control of each government department, supported by civil servants loyal to the government.
This official story provides the language that most comentators use to describe who is in charge and should be held to account. It also underpins common criticisms about how the UK political system works in practice, inclduding:
Politics is too distant from ‘the people’. Ministers make choices from the top-down, with too little regard for the wishes of the UK population.
The ‘political class’ is an elite profession, largely of white, middle or upper class, private schooled and Oxbridge educated, men. It not represent the general public
Politicians are too keen to play the ‘blame game’, hoarding power for their own benefit but blaming others when things go wrong.
Story 2. Complex government and multi-level policymaking
This story could focus on a democratic alternative. First, avoid power hoarding by sharing responsibilities with international organisations (like the European Union), devolved governments in Northern Ireland, Scotland, Wales, and English regions, and respect the electoral mandates of local governments. Indeed, perhaps this approach could aid a shift from ‘majoritarian’ towards ‘consensus’ democracy
Second, delegating policy delivery makes sense to most UK governments, seeking to set broad strategy rather than get involved in the details. Further, some organisations – such as ‘quangos’ – need some autonomy to give independent advice or proper audit of government functions.
However, policy studies tends to focus on empirical reality: how it really works, and the necessity of many policymaking centres. Here is a list of statements with links to separate posts on the underlying concepts:
Policymakers can only pay attention to a tiny proportion of their responsibilities (bounded rationality, uncertainty/ ambiguity). They pay disproportionate attention to some and ignore the rest (PET).
Policymakers delegate most issues to civil servants, who rely on specialists – including interest groups – for information and advice (policy communities).
We say ‘governance’ (not government) to describe blurry boundaries between those who have formal responsibility and informal influence over policy (MLG).
Policy problems transcend traditional government departments – like finance, health, education, justice – but policymaking is ‘fragmented’ and difficult to join-up.
Governments inherit the commitments of their predecessors, giving them limited room for manoeuvre.
If the official story is inaccurate, why does it matter and endure?
Democratic accountability via UK general elections still seems to be the ‘only game in town’, and the Westminster story seems to dominate most coverage of UK politics. Why? It provides a coherent and defendable story of who should be responsible. Even if minsters don’t live up to expectations, they still set the policy agenda and direct government resources, to benefit some groups and punish others (social construction and policy design).
It is also difficult to promote a ‘complex government’ alternative, even when decentralization seems to be inevitable and to make sense. Academics may want politicians to stop wasting their time on a misleading story, and to focus instead of managing policy pragmatically given their limitations (advice from complex systems). Yet, this story of complexity does not mix well with the Westminster story.
What happens when these stories collide?
Some ministers actually want to possess and use central powers to deliver their manifesto commitments. Some have tried to be pragmatic about their limits, but struggled to defend decentralisation. Some seem only interested in power-hoarding when they can, and blame games when they can’t. It is difficult to know what they want to do, if they can do it, and how they narrate their activities (longer discussion of King Canute).
The long-term result is a bit of a mess. There have been many public sector reforms in the name of centralising policy and decentralising delivery, including privatisation, ‘quasi-markets’, and public sector reforms (which we discuss in Chapters 4 and 5).
This mess and complexity makes the UK policy process very difficult to understand, prompting a lot of metaphors (e.g. policy communities and ‘patchwork quilts’ of delivery) or direct criticisms (e.g. the ‘incoherent state’)
Take home messages
The Westminster story remains inaccurate but important.
The complex government story is more accurate but less understandable.
It is difficult for ministers to juggle both stories (but they have to).
It has produced very different responses, and many have added to the mess.
This is a UK-centric story, but key elements have wider applicability (explored in the 500, 750, and 1000 words series).
James Nicholls, Wulf Livingston, Andy Perkins, Beth Cairns, Rebecca Foster, Kirsten M. A. Trayner, Harry R. Sumnall, Tracey Price, Paul Cairney, Josh Dumbrell, and Tessa Parkes (2022) ‘Drug Consumption Rooms and Public Health Policy: Perspectives of Scottish Strategic Decision-Makers’, International Journal of Environmental Research and Public Health, 19(11), 6575; https://doi.org/10.3390/ijerph19116575
Q: if stakeholders in Scotland express high support for drug consumption rooms, and many policymakers in Scotland seem sympathetic, why is there so little prospect of policy change?
My summary of the article’s answer is as follows:
Although stakeholders support DCRs almost unanimously, they do not support them energetically.
They see this solution as one part of a much larger package rather than a magic bullet. They are not sure of the cost-effectiveness in relation to other solutions, and can envisage some potential users not using them.
The existing evidence on their effectiveness is not persuasive for people who (1) adhere to a hierarchy of evidence which prioritizes evidence from randomized control trials or (2) advocate alternative ways to use evidence.
There are competing ways to frame this policy solution. It suggests that there are some unresolved issues among stakeholders which have not yet come to the fore (since the lack of need to implement something specific reduces the need to engage with a more concrete problem definition).
This method invites local policymakers and practitioners to try out new solutions, work with stakeholders and service users during delivery, reflect on the results, and use this learning to design the next iteration. This is a pragmatic, small-scale, approach that appeals to the (small-c conservative) Scottish Government, which uses pilots to delay major policy changes, and is keen on its image as not too centralist and quite collaboration minded.
3. This approach is not politically feasible in this case.
Some factors suggest that the general argument has almost been won, including positive informal feedback from policymakers, and increasingly sympathetic media coverage (albeit using problematic ways to describe drug use).
However, this level of support is not enough to support experimentation. Drug consumption rooms would need a far stronger steer from the Scottish Government.
In this case, it can’t experiment now and decide later. It needs to make a strong choice (with inevitable negative blowback) and stay the course, knowing that one failed political experiment could set back progress for years.
4. The multi-level policymaking system is not conducive to overcoming these obstacles.
The issue of drugs policy is often described as a public health – and therefore devolved – issue politically (and in policy circles)
However, the legal/ formal division of responsibilities suggests that UK government consent is necessary and not forthcoming.
It is possible that the Scottish Government could take a chance and act alone. Indeed, the example of smoking in public places showed that it shifted its position after a slow start (it described the issue as reserved to the UK took charge of its own legislation, albeit with UK support).
However, the Scottish Government seems unwilling to take that chance, partly because it has been stung by legal challenges in other areas, and is reluctant to engage in more of the same (see minimum unit pricing for alcohol).
Local policymakers could experiment on their own, but they won’t do it without proper authority from a central government.
This experience is part of a more general issue: people may describe multi-level policymaking as a source of venues for experimentation (‘laboratories of democracy’) to encourage policy learning and collaboration. However, this case, and cases like fracking, show that they can actually be sites of multiple veto points and multi-level reluctance.
If so, the remaining question for reflection is: what would it take to overcome these obstacles? The election of a Labour UK government? Scottish independence? Or, is there some other way to make it happen in the current context?
Update 11.9.23
There was some other way to allow a pilot to happen:
The significance of this is that when the Lord Advocate makes a statement such as the one proposed here, it bars any case covered from public prosecution. It is not simply a statement of present views which can be departed from in an individual case; it is binding until revoked. https://t.co/RXeM1kC5SW
Not really Kenny. Drugs law is reserved. Prosecution policy isn't set by Holyrood or the Scottish Government. They can't direct the Lord Advocate (nor for that matter can Westminster). If Bain had taken a different view of the public interest, we'd be stuck in the same impasse.
By James Nicholls and Paul Cairney, for the University of Stirling MPH and MPP programmes.
There are strong links between the study of public health and public policy. For example, public health scholars often draw on policy theories to help explain (often low amounts of) policy change to foster population health or reduce health inequalities. Studies include a general focus on public health strategies (such as HiAP) or specific policy instruments (such as a ban on smoking in public places). While public health scholars may seek to evaluate or influence policy, policy theories tend to focus on explaining processes and outcomes.
To demonstrate these links, we present:
A long-read blog post to (a) use an initial description of a key alcohol policy instrument (minimum unit pricing, adopted by the Scottish Government but not the UK Government) to (b) describe the application of policy concepts and theories and reflect on the empirical and practical implications. We then added some examples of further reading.
A 45 minute podcast to describe and explain these developments (click below or scroll to the end)
Minimum Unit Pricing in Scotland: background and development
Minimum Unit Pricing for alcohol was introduced in Scotland in 2018. In 2012, the UK Government had also announced plans to introduce MUP, but within a year dopped the policy following intense industry pressure. What do these two journeys tell us about policy processes?
When MUP was first proposed by Scottish Health Action on Alcohol Problems in 2007, it was a novel policy idea. Public health advocates had long argued that raising the price of alcohol could help tackle harmful consumption. However, conventional tax increases were not always passed onto consumers, so would not necessarily raise prices in the shops (and the Scottish Government did not have such taxation powers). MUP appeared to present a neat solution to this problem. It quickly became a prominent policy goal of public health advocates in Scotland and across the UK, while gaining increasing attention, and support, from the global alcohol policy community.
In 2008, the UK Minister for Health, Dawn Primarolo, had commissioned researchers at the University of Sheffield to look into links between alcohol pricing and harm. The Sheffield team developed economic models to analysis the predicted impact of different systems. MUP was included, and the ‘Sheffield Model’ would go on to play a decisive role in developing the case for the policy.
What problem would MUP help to solve?
Descriptions of the policy problem often differed in relation to each government. In the mid-2000s, alcohol harm had become a political problem for the UK government. Increasing consumption, alongside changes to the night-time economy, had started to gain widespread media attention. In 2004, just as a major liberalisation of the licensing system was underway in England, news stories began documenting the apparent horrors of ‘Binge Britain’: focusing on public drunkenness and disorder, but also growing rates of liver disease and alcohol-related hospital admissions.
In 2004, influential papers such as the Daily Mail began to target New Labour alcohol policy
Politicians began to respond, and the issue became especially useful for the Conservatives who were developing a narrative that Britain was ‘broken’ under New Labour. Labour’s liberalising reforms of alcohol licensing could conveniently be linked to this political framing. The newly formed Alcohol Health Alliance, a coalition set up under the leadership of Professor Sir Ian Gilmore, was also putting pressure on the UK Government to introduce stricter controls. In Scotland, while much of the debate on alcohol focused on crime and disorder, Scottish advocates were focused on framing the problem as one of public health. Emerging evidence showed that Scotland had dramatically higher rates of alcohol-related illness and death than the rest of Europe – a situation strikingly captured in a chart published in the Lancet.
Source: Leon, D. and McCambridge, J. (2006). Liver cirrhosis mortality rates in Britain from 1950 to 2002: an analysis of routine data. Lancet 367
The notion that Scotland faced an especially acute public health problem with alcohol was supported by key figures in the increasingly powerful Scottish National Party (in government since 2007), which, around this time, had developed working relationships with Alcohol Focus Scotland and other advocacy groups.
What happened next?
The SNP first announced that it would support MUP in 2008, but it did not implement this change until 2018. There are two key reasons for the delay:
Its minority government did not achieve enough parliamentary support to pass legislation. It then formed a majority government in 2011, and its legislation to bring MUP into law was passed in 2012.
Court action took years to resolve. The alcohol industry, which is historically powerful in Scotland, was vehemently opposed. A coalition of industry bodies, led by the Scotch Whisky Association, took the Scottish Government to court in an attempt to prove the policy was illegal. Ultimately, this process would take years, and conclude in rulings by the European Court of Justice (2016), Scottish Court of Session Inner House (2016), and UK Supreme Court (2017) which found in favour of the Scottish Government.
Once again, the alcohol industry swung into action, launching a campaign led by the Wine and Spirits Trade Association, asking ‘Why should moderate drinkers pay more?’
This public campaign was accompanied by intense behind-the-scenes lobbying, aided by the fact that the leadership of industry groups had close ties to Government and that the All-Party Parliamentary Group on Beer had the largest membership of any APPG in Westminster. The industry campaign made much of the fact there was little evidence to suggest MUP would reduce crime, but also argued strongly that the modelling produced by Sheffield University was not valid evidence in the first place. A year after the adopting the policy, the UK Government announced a U-turn and MUP was dropped.
How can we use policy theories and concepts to interpret these dynamics?
Here are some examples of using policy theories and concepts as a lens to interpret these developments.
1. What was the impact of evidence in the case for policy change?
First, many political actors (including policymakers) have many different ideas about what counts as good evidence.
The assessment, promotion, and use of evidence is highly contested, and never speaks for itself.
Second, policymakers have to ignore almost all evidence to make choices.
They address ‘bounded rationality’ by using two cognitive shortcuts: ‘rational’ measures set goals and identify trusted sources, while ‘irrational’ measures use gut instinct, emotions, and firmly held beliefs.
Third, policymakers do not control the policy process.
There is no centralised and orderly policy cycle. Rather, policymaking involves policymakers and influencers spread across many authoritative ‘venues’, with each venue having its own rules, networks, and ways of thinking.
In that context, policy theories identify the importance of contestation between policy actors, and describe the development of policy problems, and how evidence fits in. Approaches include:
The acceptability of a policy solution will often depend on how the problem is described. Policymakers use evidence to reduce uncertainty, or a lack of information around problems and how to solve them. However, politics is about exercising power to reduce ambiguity, or the ability to interpret the same problem in different ways.
By suggesting MUP would solve problems around crime, the UK Government made it easier for opponents to claim the policy wasn’t evidence-based. In Scotland, policymakers and advocates focused on health, where the evidence was stronger. In addition, the SNP’s approach fitted within a wider political independence frame, in which more autonomy meant more innovation.
Policy actors tell stories to appeal to the beliefs (or exploit the cognitive shortcuts) of their audiences. A narrative contains a setting (the policy problem), characters (such as the villain who caused it, or the victim of its effects), plot (e.g. a heroic journey to solve the problem), and moral (e.g. the solution to the problem).
Supporters of MUP tended to tell the story that there was an urgent public health crisis, caused largely by the alcohol industry, and with many victims, but that higher alcohol prices pointed to one way out of this hole. Meanwhile opponents told the story of an overbearing ‘nanny state’, whose victims – ordinary, moderate drinkers – should be left alone by government.
Policymakers make strategic and emotional choices, to identify ‘good’ populations deserving of government help, and ‘bad’ populations deserving punishment or little help. These judgements inform policy design (government policies and practices) and provide positive or dispiriting signals to citizens.
For example, opponents of MUP rejected the idea that alcohol harms existed throughout the population. They focused instead on dividing the majority of moderate drinkers from irresponsible minority of binge drinkers, suggesting that MUP would harm the former more than help the latter.
This competition to frame policy problems takes place in political systems that contain many ‘centres’, or venues for authoritative choice. Some diffusion of power is by choice, such as to share responsibilities with devolved and local governments. Some is by necessity, since policymakers can only pay attention to a small proportion of their responsibilities, and delegate the rest to unelected actors such as civil servants and public bodies (who often rely on interest groups to process policy).
For example, ‘alcohol policy’ is really a collection of instruments made or influenced by many bodies, including (until Brexit) European organisations deciding on the legality of MUP, UK and Scottish governments, as well as local governments responsible for alcohol licensing. In Scotland, this delegation of powers worked in favour of MUP, since Alcohol Focus Scotland were funded by the Scottish Government to help deliver some of their alcohol policy goals, and giving them more privileged access than would otherwise have been the case.
The role of evidence in MUP
In the case of MUP, similar evidence was available and communicated to policymakers, but used and interpreted differently, in different centres, by the politicians who favoured or opposed MUP.
In Scotland, the promotion, use of, and receptivity to research evidence – on the size of the problem and potential benefit of a new solution – played a key role in increasing political momentum. The forms of evidence were complimentary. The ‘hard’ science on a potentially effective solution seemed authoritative (although few understood the details), and was preceded by easily communicated and digested evidence on a concrete problem:
There was compelling evidence of a public health problem put forward by a well-organised ‘advocacy coalition’ (see below) which focused clearly on health harms. In government, there was strong attention to this evidence, such as the Lancet chart which one civil servant described as ‘look[ing] like the north face of the Eiger’. There were also influential ‘champions’ in Government willing to frame action as supporting the national wellbeing.
Reports from Sheffield University appeared to provide robust evidence that MUP could reduce harm, and advocacy was supported by research from Canada which suggested that similar policies there had been successful elsewhere.
Advocacy in England was also well-organised and influential, but was dealing with a larger – and less supportive – Government machine, and the dominant political frame for alcohol harms remained crime and disorder rather than health.
Debates on MUP modelling exemplify these differences in evidence communication and use. Those in favour appealed to econometric models, but sometimes simplifying their complexity and blurring the distinction between projected outcomes and proof of efficacy. Opponents went the other way and dismissed the modelling as mere speculation. What is striking is the extent to which an incredibly complex, and often poorly understand, set of econometric models – and the ’Sheffield Model’ in particular – came to occupy centre stage in a national policy debate. Katikireddi and colleagues talked about this as an example of evidence as rhetoric:
Support became less about engagement with the econometric modelling, and more an indicator of general concern about alcohol harm and the power of the industry.
Scepticism was often viewed as the ‘industry position’, and an indicator of scepticism towards public health policy more broadly.
2. Who influences policy change?
Advocacy plays a key role in alcohol policy, with industry and other actors competing with public health groups to define and solve alcohol policy problems. It prompts our attention to policy networks, or the actors who make and influence policy.
People engage in politics to turn their beliefs into policy. They form advocacy coalitions with people who share their beliefs, and compete with other coalitions. The action takes place within a subsystem devoted to a policy issue, and a wider policymaking process that provides constraints and opportunities to coalitions. Beliefs about how to interpret policy problems act as a glue to bind actors together within coalitions. If the policy issue is technical and humdrum, there may be room for routine cooperation. If the issue is highly charged, then people romanticise their own cause and demonise their opponents.
MUP became a highly charged focus of contestation between a coalition of public health advocates, who saw themselves as fighting for the wellbeing of the wider community (and who believed fundamentally that government had a duty to promote population health), and a coalition of industry actors who were defending their commercial interests, while depicting public health policies as illiberal and unfair.
3. Was there a ‘window of opportunity’ for MUP?
Policy theories – including Punctuated Equilibrium Theory – describe a tendency for policy change to be minor in most cases and major in few. Paradigmatic policy change is rare and may take place over decades, as in the case of UK tobacco control where many different policy instruments changed from the 1980s. Therefore, a major change in one instrument could represent a sea-change overall or a modest adjustment to the overall approach.
Multiple Streams Analysis is a popular way to describe the adoption of a new policy solution such as MUP. It describes disorderly policymaking, in which attention to a policy problem does not produce the inevitable development, implementation, and evaluation of solutions. Rather, these ‘stages’ should be seen as separate ‘streams’. A ‘window of opportunity’ for policy change occurs when the three ‘streams’ come together:
Problem stream. There is high attention to one way to define a policy problem.
Policy stream. A technically and politically feasible solution already exists (and is often pushed by a ‘policy entrepreneur’ with the resources and networks to exploit opportunities).
Politics stream. Policymakers have the motive and opportunity to choose that solution.
However, these windows open and close, often quickly, and often without producing policy change.
This approach can help to interpret different developments in relation to Scottish and UK governments:
Problem stream
The Scottish Government paid high attention to public health crises, including the role of high alcohol consumption.
The UK government paid often-high attention to alcohol’s role in crime and anti-social behaviour (‘Binge Britain’ and ‘Broken Britain’)
Policy stream
In Scotland, MUP connected strongly to the dominant framing, offering a technically feasible solution that became politically feasible in 2011.
The UK Prime Minister David Cameron’s made a surprising bid to adopt MUP in 2012, but ministers were divided on its technical feasibility (to address the problem they described) and its political feasibility seemed to be more about distracting from other crises than public health.
Politics stream
The Scottish Government was highly motivated to adopt MUP. MUP was a flagship policy for the SNP; an opportunity to prove its independent credentials, and to be seen to address a national public health problem. It had the opportunity from 2011, then faced interest group opposition that delayed implementation.
The Coalition Government was ideologically more committed to defending commercial interests, and to framing alcohol harms as one of individual (rather than corporate) responsibility. It took less than a year for the alcohol industry to successfully push for a UK government U-turn.
As a result, MUP became policy (eventually) in Scotland, but the window closed (without resolution) in England.
Paul Cairney and Donley Studlar (2014) ‘Public Health Policy in the United Kingdom: After the War on Tobacco, Is a War on Alcohol Brewing?’ World Medical and Health Policy, 6, 3, 308-323PDF
Niamh Fitzgerald and Paul Cairney (2022) ‘National objectives, local policymaking: public health efforts to translate national legislation into local policy in Scottish alcohol licensing’, Evidence and Policy, https://doi.org/10.1332/174426421X16397418342227, PDF
Podcast
You can listen directly here:
You can also listen on Spotify or iTunes via Anchor
By James Nicholls and Paul Cairney, for the University of Stirling MPH and MPP programmes.
There are strong links between the study of public health and public policy. For example, public health scholars often draw on policy theories to help explain (often low amounts of) policy change to foster population health or reduce health inequalities. Studies include a general focus on public health strategies (such as HiAP) or specific policy instruments (such as a ban on smoking in public places). While public health scholars may seek to evaluate or influence policy, policy theories tend to focus on explaining processes and outcomes,.
To demonstrate these links, we present this podcast and blog post to (1) use an initial description of a key alcohol policy instrument (minimum unit pricing in Scotland) to (2) describe the application of policy concepts and theories and reflect on the empirical and practical implications.
Using policy theories to interpret public health case studies: the example of a minimum unit price for alcohol | Paul Cairney: Politics & Public Policy (wordpress.com)
In the summer of 2020, after cancelling exams, the UK and devolved governments sought teacher estimates on students’ grades, but supported an algorithm to standardise the results. When the results produced a public outcry over unfair consequences, they initially defended their decision but reverted quickly to teacher assessment. These experiences, argue Sean Kippin and Paul Cairney, highlight the confluence of events and choices in which an imperfect and rejected policy solution became a ‘lifeline’ for four beleaguered governments.
In 2020, the UK and devolved governments performed a ‘U-turn’ on their COVID-19 school exams replacement policies. The experience was embarrassing for education ministers and damaging to students. There are significant differences between (and often within) the four nations in terms of the structure, timing, weight, and relationship between the different examinations. However, in general, the A-level (England, Northern Ireland, Wales) and Higher/ Advanced Higher (Scotland) examinations have similar policy implications, dictating entry to further and higher education, and influencing employment opportunities. The Priestley review, commissioned by the Scottish Government after their U-turn, described this as an ‘impossible task’.
Initially, each government defined the new policy problem in relation to the need to ‘credibly’ replicate the purpose of exams to allow students to progress to tertiary education or employment. All four quickly announced their intentions to allocate in some form grades to students, rather than replace the assessments with, for example, remote examinations. However, mindful of the long-term credibility of the examinations system and of ensuring fairness, each government opted to maintain the qualifications and seek a similar distribution of grades to previous years. A key consideration was that UK universities accept large numbers of students from across the UK.
One potential solution open to policymakers was to rely solely on teacher grading (CAG). CAGs are ‘based on a range of evidence including mock exams, non-exam assessment, homework assignments and any other record of student performance over the course of study’. Potential problems included the risk of high variation and discrepancies between different centres, the potential overload of the higher education system, and the tendency for teacher predicted grades to reward already privileged students and punish disabled, non-white, and economically deprived children.
A second option was to take CAGs as a starting point, then use an algorithm to produce ‘standardisation’, which was potentially attractive to each government as it allowed students to complete secondary education and to progress to the next level in similar ways to previous (and future) cohorts. Further, an emphasis on the technical nature of this standardisation, with qualifications agencies taking the lead in designing the process by which grades would be allocated, and opting not share the details of its algorithm were a key part of its (temporary) viability. Each government then made similar claims when defending the problem and selecting the solution. Yet this approach reduced both the debate on the unequal impact of this process on students, and the chance for other experts to examine if the algorithm would produce the desired effect. Policymakers in all four governments assured students that the grading would be accurate and fair, with teacher discretion playing a large role in the calculation of grades.
To these governments, it appeared at first that they had found a fair and efficient (or at least defendable) way to allocate grades, and public opinion did not respond negatively to its announcement. However, these appearances proved to be profoundly deceptive and vanished on each day of each exam result. The Scottish national mood shifted so intensely that, after a few days, pursuing standardisation no longer seemed politically feasible. The intense criticism centred on the unequal level of reductions of grades after standardisation, rather than the unequal overall rise in grade performance after teacher assessment and standardisation (which advantaged poorer students).
Despite some recognition that similar problems were afoot elsewhere, this shift of problem definition did not happen in the rest of the UK until (a) their published exam results highlighted similar problems regarding the role of previous school performance on standardised results, and (b) the Scottish Government had already changed course. Upon the release of grades outside Scotland, it became clear that downgrades were also concentrated in more deprived areas. For instance, in Wales, 42% of students saw their A-Level results lowered from their Centre Assessed Grades, with the figure close to a third for Northern Ireland.
Each government thus faced similar choices between defending the original system by challenging the emerging consensus around its apparent unfairness; modifying the system by changing the appeal system; or abandoning it altogether and reverting to solely teacher assessed grades. Ultimately, all three governments followed the same path. Initially, they opted to defend their original policy choice. However, by 17 August, the UK, Welsh, and Northern education secretaries announced (separately) that examination grades would be based solely on CAGs – unless the standardisation process had generated a higher grade (students would receive whichever was highest).
Scotland’s initial experience was instructive to the rest of the UK and its example provided the UK government with a blueprint to follow (eventually). It began with a new policy choice – reverting to teacher assessed grades – sold as fairer to victims of the standardisation process. Once this precedent had been set, a different course for policymakers at the UK level became difficult to resist, particularly when faced with a similar backlash. The UK’s government’s decision in turn influenced the Welsh and Northern Irish governments.
In short, we can see that the particular ordering of choices created a cascading effect across the four governments which created initially one policy solution, before triggering a U-turn. This focus on order and timing should not be lost during the inevitable inquiries and reports on the examinations systems. The take-home message is to not ignore the policy process when evaluating the long-term effect of these policies. Focus on why the standardisation processes went wrong is welcome, but we should also focus on why the policymaking process malfunctioned, to produce a wildly inconsistent approach to the same policy choice in such a short space of time. Examining both aspects of this fiasco will be crucial to the grading process in 2021, given that governments will be seeking an alternative to exams for a second year.
__________________________
Note: the above draws on the authors’ published work in British Politics.
This post first appeared on LSE British Politics and Policy (27.11.20) and is based on this article in British Politics.
Paul Cairneyassesses government policy in the first half of 2020. He identifies the intense criticism of its response so far, encouraging more systematic assessments grounded in policy research.
In March 2020, COVID-19 prompted policy change in the UK at a speed and scale only seen during wartime. According to the UK government, policy was informed heavily by science advice. Prime Minister Boris Johnson argued that, ‘At all stages, we have been guided by the science, and we will do the right thing at the right time’. Further, key scientific advisers such as Sir Patrick Vallance emphasised the need to gather evidence continuously to model the epidemic and identify key points at which to intervene, to reduce the size of the peak of population illness initially, then manage the spread of the virus over the longer term.
Both ministers and advisors emphasised the need for individual behavioural change, supplemented by government action, in a liberal democracy in which direct imposition is unusual and unsustainable. However, for its critics, the government experience has quickly become an exemplar of policy failure.
Initial criticisms include that ministers did not take COVID-19 seriously enough in relation to existing evidence, when its devastating effect was apparent in China in January and Italy from February; act as quickly as other countries to test for infection to limit its spread; or introduce swift-enough measures to close schools, businesses, and major social events. Subsequent criticisms highlight problems in securing personal protective equipment (PPE), testing capacity, and an effective test-trace-and-isolate system. Some suggest that the UK government was responding to the ‘wrong pandemic’, assuming that COVID-19 could be treated like influenza. Others blame ministers for not pursuing an elimination strategy to minimise its spread until a vaccine could be developed. Some criticise their over-reliance on models which underestimated the R (rate of transmission) and ‘doubling time’ of cases and contributed to a 2-week delay of lockdown. Many describe these problems and delays as the contributors to the UK’s internationally high number of excess deaths.
How can we hold ministers to account in a meaningful way?
I argue that these debates are often fruitless and too narrow because they do not involve systematic policy analysis, take into account what policymakers can actually do, or widen debate to consider whose lives matter to policymakers. Drawing on three policy analysis perspectives, I explore the questions that we should ask to hold ministers to account in a way that encourages meaningful learning from early experience.
These questions include:
Was the government’s definition of the problem appropriate? Much analysis of UK government competence relates to specific deficiencies in preparation (such as shortages in PPE), immediate action (such as to discharge people from hospitals to care homes without testing them for COVID-19), and implementation (such as an imperfect test-trace-and-isolate system). The broader issue relates to its focus on intervening in late March to protect healthcare capacity during a peak of infection, rather than taking a quicker and more precautionary approach. This judgment relates largely to its definition of the policy problem which underpins every subsequent policy intervention.
Did the government select the right policy mix at the right time? Who benefits most from its choices?
Most debates focus on the ‘lock down or not?’ question without exploring fully the unequal impact of any action. The government initially relied on exhortation, based on voluntarism and an appeal to social responsibility. Initial policy inaction had unequal consequences on social groups, including people with underlying health conditions, black and ethnic minority populations more susceptible to mortality at work or discrimination by public services, care home residents, disabled people unable to receive services, non-UK citizens obliged to pay more to live and work while less able to access public funds, and populations (such as prisoners and drug users) that receive minimal public sympathy. Then, in March, its ‘stay at home’ requirement initiated a major new policy and different unequal impacts in relation to the income, employment, and wellbeing of different groups. These inequalities are list in more general discussions of impacts on the whole population.
Did the UK government make the right choices on the trade-offs between values, and what impacts could the government have reasonably predicted?
Initially, the most high-profile value judgment related to freedom from state coercion to reduce infection versus freedom from the harm of infection caused by others. Then, values underpinned choices on the equitable distribution of measures to mitigate the economic and wellbeing consequences of lockdown. A tendency for the UK government to project centralised and ‘guided by the science’ policymaking has undermined public deliberation on these trade-offs between policies. The latter will be crucial to ongoing debates on the trade-offs associated with national and regional lockdowns.
Did the UK government combine good policy with good policymaking?
A problem like COVID-19 requires trial-and-error policymaking on a scale that seems incomparable to previous experiences. It requires further reflection on how to foster transparent and adaptive policymaking and widespread public ownership for unprecedented policy measures, in a political system characterised by (a) accountability focused incorrectly on strong central government control and (b) adversarial politics that is not conducive to consensus seeking and cooperation.
These additional perspectives and questions show that too-narrow questions – such as was the UK government ‘following the science’ – do not help us understand the longer term development and wider consequences of UK COVID-19 policy. Indeed, such a narrow focus on science marginalises wider discussions of values and the populations that are most disadvantaged by government policy.
This post first appeared as Who controls public policy? on the UK in a Changing Europe website. There is also a 1-minute video, but you would need to be a completist to want to watch it.
Our #AcademicintheSpotlight series highlights social scientists doing innovative & dynamic research that you really ought to be aware of.
This week, it’s the turn of @CairneyPaul. Paul works on understanding the mechanics of public policy and policymaking. Interested? Read on… pic.twitter.com/bMs8RoQi2a
Most coverage of British politics focuses on the powers of a small group of people at the heart of government. In contrast, my research on public policy highlights two major limits to those powers, related to the enormous number of problems that policymakers face, and to the sheer size of the government machine.
First, elected policymakers simply do not have the ability to properly understand, let alone solve, the many complex policy problems they face. They deal with this limitation by paying unusually high attention to a small number of problems and effectively ignoring the rest.
Second, policymakers rely on a huge government machine and network of organisations (containing over 5 million public employees) essential to policy delivery, and oversee a statute book which they could not possibly understand.
In other words, they have limited knowledge and even less control of the state, and have to make choices without knowing how they relate to existing policies (or even what happens next).
These limits to ministerial powers should prompt us to think differently about how to hold them to account. If they only have the ability to influence a small proportion of government business, should we blame them for everything that happens in their name?
My approach is to apply these general insights to specific problems in British politics. Three examples help to illustrate their ability to inform British politics in new ways.
First, policymaking can never be ‘evidence based’. Some scientists cling to the idea that the ‘best’ evidence should always catch the attention of policymakers, and assume that ‘speaking truth to power’ helps evidence win the day.
As such, researchers in fields like public health and climate change wonder why policymakers seem to ignore their evidence.
The truth is that policymakers only have the capacity to consider a tiny proportion of all available information. Therefore, they must find efficient ways to ignore almost all evidence to make timely choices.
They do so by setting goals and identifying trusted sources of evidence, but also using their gut instinct and beliefs to rule out most evidence as irrelevant to their aims.
Second, the UK government cannot ‘take back control’ of policy following Brexit simply because it was not in control of policy before the UK joined. The idea of control is built on the false image of a powerful centre of government led by a small number of elected policymakers.
This way of thinking assumes that sharing power is simply a choice. However, sharing power and responsibility is borne of necessity because the British state is too large to be manageable.
Governments manage this complexity by breaking down their responsibilities into many government departments. Still, ministers can only pay attention to a tiny proportion of issues managed by each department. They delegate most of their responsibilities to civil servants, agencies, and other parts of the public sector.
In turn, those organisations rely on interest groups and experts to provide information and advice.
As a result, most public policy is conducted through small and specialist ‘policy communities’ that operate out of the public spotlight and with minimal elected policymaker involvement.
The logical conclusion is that senior elected politicians are less important than people think. While we like to think of ministers sitting in Whitehall and taking crucial decisions, most of these decisions are taken in their name but without their intervention.
Third, the current pandemic underlines all too clearly the limits of government power. Of course people are pondering the degree to which we can blame UK government ministers for poor choices in relation to Covid-19, or learn from their mistakes to inform better policy.
Many focus on the extent to which ministers were ‘guided by the science’. However, at the onset of a new crisis, government scientists face the same uncertainty about the nature of the policy problem, and ministers are not really able to tell if a Covid-19 policy would work as intended or receive enough public support.
Some examples from the UK experience expose the limited extent to which policymakers can understand, far less control, an emerging crisis.
Prior to the lockdown, neither scientists nor ministers knew how many people were infected, nor when levels of infection would peak.
They had limited capacity to test. They did not know how often (and how well) people wash their hands. They did not expect people to accept and follow strict lockdown rules so readily, and did not know which combination of measures would have the biggest impact.
When supporting businesses and workers during ‘furlough’, they did not know who would be affected and therefore how much the scheme would cost.
In short, while Covid-19 has prompted policy change and state intervention on a scale not witnessed outside of wartime, the government has never really known what impact its measures would have.
Overall, the take-home message is that the UK narrative of strong central government control is damaging to political debate and undermines policy learning. It suggests that every poor outcome is simply the consequence of bad choices by powerful leaders. If so, we are unable to distinguish between the limited competence of some leaders and the limited powers of them all.
SAGE’s emphasis on uncertainty and limited knowledge extended to the evidence on how to influence behaviour via communication:
‘there is limited evidence on the best phrasing of messages, the barriers and stressors that people will encounter when trying to follow guidance, the attitudes of the public to the interventions, or the best strategies to promote adherence in the long-term’ (SPI-B Meeting paper 3.3.20: 2)
Early on, SAGE minutes described continuously the potential problems of communicating risk and encouraging behavioural change through communication (in other words, based on low expectations for the types of quarantine measures associated with China and South Korea).
It sought ‘behavioural science input on public communication’ and ‘agreed on the importance of behavioural science informing policy – and on the importance of public trust in HMG’s approach’ (28.1.20: 2).
It worried about how the public might interpret ‘case fatality rate’, given the different ways to describe and interpret frequencies and risks (4.2.20: 3).
It stated that ‘Epidemiological terms need to be made clearer in the planning documents to avoid ambiguity’ (11.2.20: 3).
Its extensive discussion of behavioural science (13.2.20: 2-3) includes: there will be public scepticism and inaction until first deaths are confirmed; the main aim is to motivate people by relating behavioural change to their lives; messaging should stress ‘personal responsibility and responsibility to others’ and be clear on which measures are effective’, and ‘National messaging should be clear and definitive: if such messaging is presented as both precautionary and sufficient, it will reduce the likelihood of the public adopting further unnecessary or contradictory behaviours’ (13.2.20: 2-3)
Banning large public events could signal the need to change behaviour more generally, but evidence for its likely impact is unavailable (SPI-M-O, 11.2.20: 1).
Generally speaking, the assumption underpinning communication is that behavioural change will come largely from communication (encouragement and exhortation) rather than imposition. Hence, for example, the SPI-B (25.2.20: 2) recommendation on limiting the ‘risk of public disorder’:
‘Provide clear and transparent reasons for different strategies: The public need to understand the purpose of the Government’s policy, why the UK approach differs to other countries and how resources are being allocated. SPI-B agreed that government should prioritise messaging that explains clearly why certain actions are being taken, ahead of messaging designed solely for reassuring the public.
This should also set clear expectations on how the response will develop, g. ensuring the public understands what they can expect as the outbreak evolves and what will happen when large numbers of people present at hospitals. The use of early messaging will help, as a) individuals are likely to be more receptive to messages before an issue becomes controversial and b) it will promote a sense the Government is following a plan.
Promote a sense of collectivism: All messaging should reinforce a sense of community, that “we are all in this together.” This will avoid increasing tensions between different groups (including between responding agencies and the public); promote social norms around behaviours; and lead to self-policing within communities around important behaviours’.
The underpinning assumption is that the government should treat people as ‘rational actors’: explain risk and how to reduce it, support existing measures by the public to socially distance, be transparent, explain if UK is doing things differently to other countries, and recognise that these measures are easier for some more than others (13.3.20: 3).
In that context, SPI-B Meeting paper 22.3.20 describes how to enable social distancing with reference to the ‘behaviour change wheel’ (Michie et al, 2011): ‘There are nine broad ways of achieving behaviour change: Education, Persuasion, Incentivisation, Coercion, Enablement, Training, Restriction, Environmental restructuring, and Modelling’ and many could reinforce each other (22.3.20: 1). The paper comments on current policy in relation to 5 elements:
Education – clarify guidance (generally, and for shielding), e.g. through interactive website, tailored to many audiences
Persuasion – increase perceived threat among ‘those who are complacent, using hard-hitting emotional messaging’ while providing clarity and positive messaging (tailored to your audience’s motivation) on what action to take (22.3.20: 1-2).
Incentivisation – emphasise social approval as a reward for behaviour change
Coercion – ‘Consideration should be given to enacting legislation, with community involvement, to compel key social distancing measures’ (combined with encouraging ‘social disapproval but with a strong caveat around unwanted negative consequences’ (22.3.20: 2)
Enablement – make sure that people have alternative access to social contact, food, and other resources for people feeling the unequal impact of lockdown (particularly for vulnerable people shielding, aided by community support).
Apparently, section 3 of SPI-B’s meeting paper (1.4.20b: 2) had been redacted because it was critical of a UK Government ‘Framework; with 4 new proposals for greater compliance: ‘17) increasing the financial penalties imposed; 18) introducing self-validation for movements; 19) reducing exercise and/or shopping; 20) reducing non-home working’. On 17, it suggests that the evidence base for (e.g.) fining someone exercising more than 1km from their home could contribute to lower support for policy overall. On 17-19, it suggests that most people are already complying, so there is no evidence to support more targeted measures. It is more positive about 20, since it could reduce non-home working (especially if financially supported). Generally, it suggests that ministers should ‘also consider the role of rewards and facilitations in improving adherence’ and use organisational changes, such as staggered work hours and new use of space, rather than simply focusing on individuals.
Communication after the lockdown
SAGE suggests that communication problems are more complicated during the release of lockdown measures (in other words, without the ability to present the relatively-low-ambiguity message ‘stay at home’). Examples (mostly from SPI-B and its contributors) include:
When notifying people about the need to self-isolate, address the trade-offs between symptom versus positive test based notifications (meeting paper 29.4.20a: 1-4; 5.5.20: 1-8)
If you are worried about public ‘disorder’, focus on clear, effective, tailored communication, using local influencers, appealing to sympathetic groups (like NHS staff), and co-producing messages between the police and public (in other words, police via consent, and do not exacerbate grievances) (meeting papers 19.4.20: 1-4; 21.4.20: 1-3; 4.5.20: 1-11)
Be wary of lockdowns specific to very small areas, which undermine the ‘all in it together’ message (REDACTED and Clifford Stott, no date: 1). If you must to it, clarify precisely who is affected and what they should do, support the people most vulnerable and impacted (e.g. financially), and redesign physical spaces (meeting paper SPI-B 22.4.20a)
When reopening schools (fully or partly), communication is key to the inevitably complex and unpredictable behavioural consequences (so, for example, work with parents, teachers, and other stakeholders to co-produce clear guidance) (29.4.20d: 1-10)
On the introduction of Alert Levels, as part of the Joint Biosecurity Centre work on local outbreaks (described in meeting paper 20.5.20a: 1-9): build public trust and understanding regarding JBC alert levels, and relate them very clearly to expected behaviour (SAGE 28.5.20). Each Alert Level should relate clearly to a required response in that area, and ‘public communications on Alert Levels needs many trusted messengers giving the same advice, many times’ (meeting paper 27.5.20b: 3).
On transmission between social networks, ‘Communicate two key principles: 1. People whose work involves large numbers of contacts with different people should avoid close, prolonged, indoor contact with anyone as far as possible … 2. People with different workplace networks should avoid meeting or sharing the same spaces’ (meeting paper 27.5.20b: 1).
On outbreaks in ‘forgotten institutional settings’ (including Prisons, Homeless Hostels, Migrant dormitories, and Long stay mental health): address the unusually low levels of trust in (or awareness of) government messaging among so-called ‘hard to reach groups’ (meeting paper 28.5.20a: 1).
See also:
SPI-M (Meeting paper 17.3.20b: 4) list of how to describe probabilities. This is more important than it looks, since there is a potentially major gap between the public and advisory group understanding of words like ‘probably’ (compare with the CIA’s Words of Estimative Probability).
These posts introduce you to key concepts in the study of public policy. They are all designed to turn a complex policymaking world into something simple enough to understand. Some of them focus on small parts of the system. Others present ambitious ways to explain the system as a whole. The wide range of concepts should give you a sense of a variety of studies out there, but my aim is to show you that these studies have common themes.